

診察時間
午前9:00-12:00
午後15:00-18:00
手術時間12:00-15:00
水曜・日曜午後休診

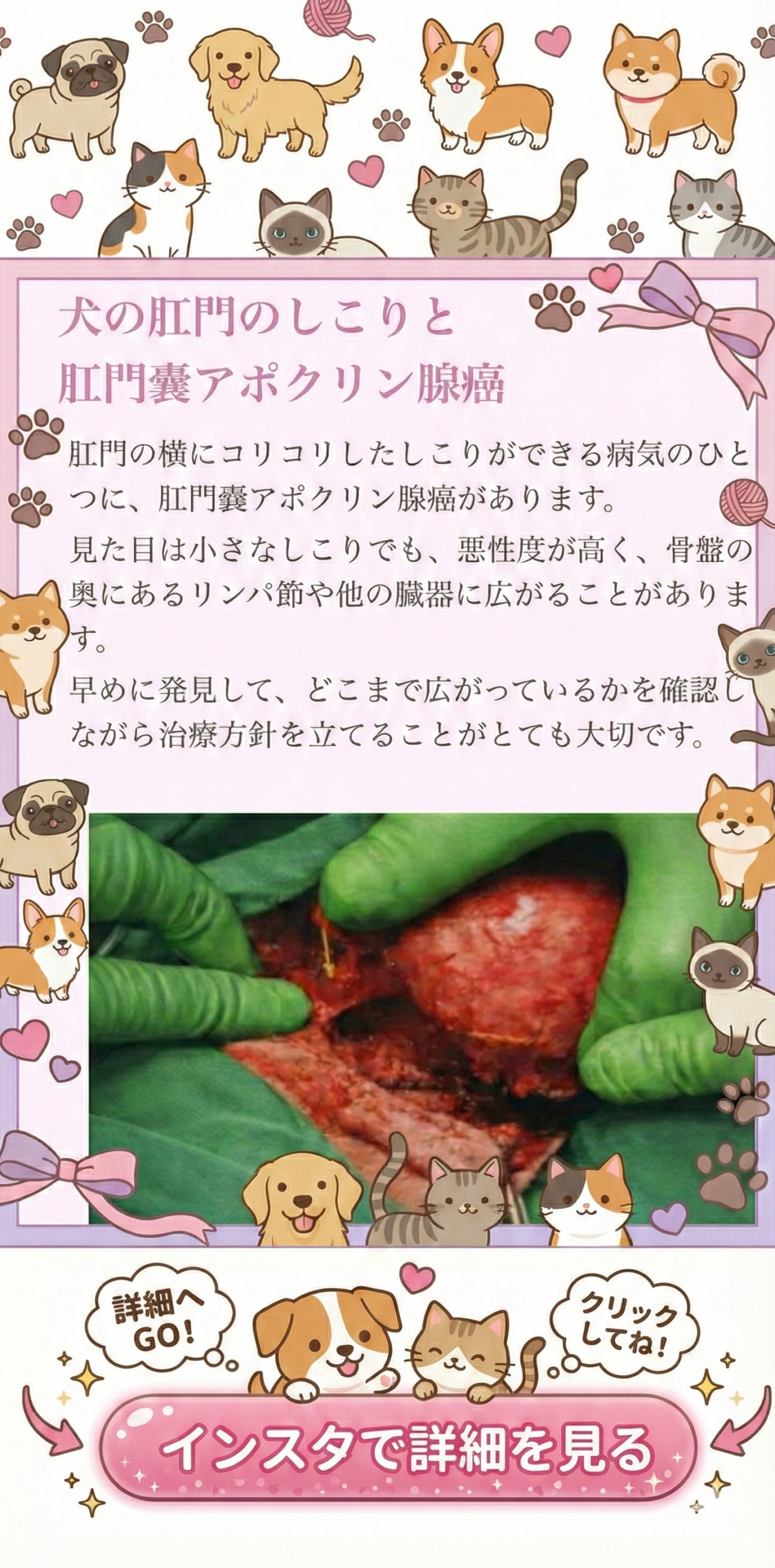
犬の肛門のしこり 肛門嚢アポクリン腺癌の検査と治療
肛門の横にできる「しこり」や、肛門まわりの腫れ・出血が気になるとき──その原因のひとつに、肛門嚢(こうもんのう)にできる腫瘍があります。
この記事でわかること
肛門嚢アポクリン腺癌(こうもんのうアポクリンせんがん)という病気の概要、検査の流れ、治療(手術・リンパ節の治療・追加治療)、麻酔のリスク、術後の見通しとご自宅でのケア、合併症や予後について、できるだけわかりやすくまとめます。
※「しこり=すぐに命に関わる」と決めつけず、でも「様子見でよい」とも言い切れません。早めの評価で治療の選択肢が広がります。
肛門嚢アポクリン腺癌とは
肛門の左右にある「肛門嚢(肛門腺)」の中には、分泌物をつくる腺があり、そこから発生する腫瘍が肛門嚢アポクリン腺癌です。犬で多い腫瘍のひとつで、肛門の横のしこりとして見つかることがあります。見た目が小さくても、体の奥にあるリンパ節(とくに骨盤の奥のリンパ節)が腫れているケースがあり、病気の広がり(病期)を丁寧に確認することがとても大切です。
どんな症状が出るの?
- 肛門の横のしこり、腫れ、出血、ただれ
- お尻を気にする、なめる、痛がる、座り方が変
- 便が細い・出しづらい、いきむ(骨盤内のリンパ節が大きいと起こりやすい)
- 元気食欲の低下(痛み・感染・全身状態の変化によることがあります)
- 多飲多尿、食欲不振、吐き気、元気消失(血液中のカルシウムが上がる「高カルシウム血症」が関係する場合があります)
ポイント:肛門周囲のしこりは「良性の炎症」や「肛門嚢の感染」でも起こりますが、見た目だけで判断できません。触診と検査で「腫瘍かどうか」「広がりがあるか」を確認します。
検査は何をするの?(診断と病期判定)
治療方針を決めるために、まず「腫瘍かどうか」「どこまで広がっているか」「麻酔・手術に耐えられる体調か」を確認します。一般的には次の流れで進みます。
- 視診・触診:肛門の左右、皮膚の状態、痛み、腫れの範囲を確認します。直腸内からの触診で、骨盤内のリンパ節の腫れや直腸の圧迫を評価します。
- 細胞診(針で細胞を取る検査):しこりから細胞を採取し、腫瘍の可能性を評価します。状況により組織検査(生検や手術で摘出して病理検査)で確定診断を行います。
- 血液検査・尿検査:炎症や貧血、肝腎機能、電解質の確認に加え、カルシウム値を含めて全身状態を評価します。高カルシウム血症がある場合は、治療と麻酔計画に影響します。
- 画像検査(胸部レントゲン/腹部超音波/CTなど):肺転移の有無、骨盤内リンパ節(内腸骨下リンパ節など)の腫大、周囲組織への浸潤の程度を確認します。骨盤の奥のリンパ節はCTで評価しやすいため、手術計画に役立つことが多いです。
- 心臓評価(必要に応じて):高齢の子や心雑音がある子では、心エコーや心電図で麻酔リスクを下げる工夫をします。
治療の選択肢(いちばん大切なのは「広がりの評価」)
肛門嚢アポクリン腺癌は、局所(肛門のしこり)だけでなく、骨盤内リンパ節への転移が見つかることがあります。治療は「局所を取る治療」と「転移や再発に備える治療」を組み合わせて考えます。
- 手術(肛門嚢の腫瘍を摘出):可能であれば第一選択になることが多い治療です。腫瘍を取り切ること(外科的マージンの確保)を目指します。
- 骨盤内リンパ節の治療(摘出・生検、または放射線など):リンパ節が腫れている場合、腫大リンパ節の治療が予後に影響します。
- 補助療法(抗がん剤、分子標的薬、放射線治療など):病理結果や病期、再発リスクに応じて検討します。
- 緩和治療:手術が難しい場合や体力的に負担が大きい場合は、痛みや排便のしにくさを和らげることを優先します。
ここが重要:腫瘍を取るだけでなく、骨盤内リンパ節の状態を一緒に評価して、必要なら同時に治療することで、長期的なコントロールにつながります。
麻酔のリスクは?(安全に受けるために)
全身麻酔には必ずリスクがありますが、事前検査と麻酔計画、術中モニター、術後管理でリスクをできるだけ下げていきます。肛門嚢アポクリン腺癌で特に注意したいポイントは、全身状態の評価(脱水、貧血、感染、腎機能・肝機能)に加えて、カルシウム値が高い場合の対応です。高カルシウム血症があると、食欲不振や脱水、腎臓への負担、心臓への影響が出ることがあるため、必要に応じて点滴などで状態を整えてから手術に臨みます。
また、肛門の近くは血流が豊富で、手術中に出血しやすい部位です。そのため、術中は確実な止血操作とモニター管理が重要になります。
手術後の流れ(入院・通院・ご自宅ケア)
術後は、痛みを抑えながら、創部(傷)と排便の状態を安定させることが最優先です。一般的には、術後数日は腫れや違和感が出やすく、排便がスムーズにいかないこともあります。病院では、痛み止め、必要に応じて抗菌薬、点滴、排便を助ける管理(便を柔らかくする薬や食事調整など)を行います。
ご自宅では、エリザベスカラーでなめるのを防ぎ、清潔を保ちながら、排便の回数・硬さ・いきみ具合、出血や腫れの変化を観察します。肛門まわりはどうしても汚れやすいので、獣医師の指示に沿って、優しく拭き取ったり洗浄したりしながら管理します。
- 術後は一時的に「便が出にくい」「いきむ」ことがあります。痛み・腫れ・緊張が原因のこともありますが、強いいきみが続く場合は早めに受診してください。
- 出血が増える、強い腫れ、膿、強い痛み、元気食欲の低下、発熱が疑われるときは、すぐに病院へ連絡してください。
- 抜糸の時期は傷の場所や縫い方で異なります。診察時に傷の状態を見て判断します。
合併症(起こりうること)
肛門周囲の手術は、場所の特性上、合併症がゼロにはできません。だからこそ、術式の選択、丁寧な組織操作、確実な止血、術後管理がとても重要です。起こりうる合併症としては、創部感染、腫れ(漿液腫)、出血、傷の開き、排便時の痛みや便秘、肛門周囲の違和感などが挙げられます。状況によっては、直腸の損傷や狭窄、排便機能への影響が問題になることもあるため、手術前にリスクを把握し、術後も丁寧にフォローします。
術後に特に気をつけたいサイン:出血が止まらない/急に腫れが強くなる/強い痛みが続く/便が全く出ない・何度もいきむ/元気食欲が落ちる──これらは早めの再診が必要なことがあります。
予後(どれくらい良くなる?)
予後は「腫瘍の大きさ」「病理結果(悪性度や切除縁)」「リンパ節転移の有無」「転移の範囲」「治療の組み合わせ(手術+リンパ節治療+補助療法)」などで変わります。肛門嚢アポクリン腺癌は、局所が小さく見えても骨盤内リンパ節が腫れていることがあるため、治療前の画像評価がとても重要です。
治療がうまくいくと、しこりによる痛みや出血、排便のしづらさが改善し、生活の質が上がることが期待できます。一方で、再発や転移の可能性がある腫瘍でもあるため、治療後も定期的なチェックが必要です。フォローの頻度は病期や治療内容により変わりますが、一定の間隔で身体検査と血液検査、必要に応じて画像検査を行い、早期の変化を拾い上げます。
追加治療について(状況により検討します)
病理検査の結果やリンパ節の状態によっては、再発や転移のリスクを下げる目的で追加治療を検討します。代表的には抗がん剤治療、分子標的薬(例:トセラニブなど)、放射線治療などがあります。どれが適切かは、病期、持病、年齢、生活スタイル、通院可能性なども含めて一緒に相談しながら決めていきます。
また、術後に傷のケアや排便管理が難しい場合、あるいは感染リスクが高い場合には、創部管理の工夫(ドレーンの使用など)を行うことがあります。必要な場合は、術前にその可能性も含めてご説明します。
よくあるご質問
- 「肛門の横のしこり」は様子見でいいですか?
炎症や感染のこともありますが、腫瘍の場合は早い段階での評価がとても大切です。まずは触診と検査で原因を確認しましょう。 - 手術をすると排便ができなくなりますか?
手術後は一時的に違和感や痛みで排便が難しいことがありますが、多くは管理で落ち着きます。ただし、腫瘍の場所や大きさ、周囲組織との関係によってはリスクが上がることがあり、術前評価と術式の工夫が重要です。 - 骨盤の奥のリンパ節が腫れていると言われました
骨盤内リンパ節の腫大は、この腫瘍で特に重要な所見です。CTなどで位置関係を確認し、摘出や追加治療の適応を検討します。 - 治療後はどれくらい通院しますか?
術後の傷のチェック、病理結果の説明、必要に応じた追加治療の相談、その後の定期検診が必要です。病期や治療内容で通院間隔は変わります。
写真を後で追加したい方へ(差し替えしやすい置き場)
この位置に、検査画像や手術写真、模式図などを後から追加できます。文章の流れが崩れにくいように、ここを「画像のまとめ置き場」として使っても大丈夫です。
画像の直前に短い説明文を入れると、読者さんにとって理解しやすくなります。
もし「どの画像をどの章の近くに置くとわかりやすいか」も一緒に整えたい場合は、画像を貼る予定の順番だけ教えていただければ、本文側の配置案も作れます。
まとめ
- 肛門嚢アポクリン腺癌は、肛門の横のしこりとして見つかることがあり、骨盤内リンパ節への転移が関わることがあります。
- 治療は、局所の手術に加えて、リンパ節の評価と必要な治療を組み合わせて考えます。
- 麻酔は事前検査と計画でリスクを下げられます。カルシウム値が高い場合は特に丁寧な全身管理が重要です。
- 術後は傷の管理と排便の観察が大切で、異変があれば早めの連絡が安心につながります。
If you notice a “lump” next to your dog’s anus, swelling around the anal area, or bleeding—one possible cause is a tumor arising from the anal sacs.
What you’ll learn in this article
This is an owner-friendly guide to Anal Sac Apocrine Gland Adenocarcinoma (ASAGAC): what it is, the typical diagnostic workup, treatment options (surgery, lymph node management, additional therapy), anesthesia considerations, the post-operative plan and home care, possible complications, and prognosis—so you can understand the condition even without reading the original papers.
A key message: a lump is not automatically “life-threatening right away,” but it is also not something we can safely label as “okay to watch” without proper evaluation. Earlier assessment often means more options.
What is Anal Sac Apocrine Gland Adenocarcinoma (ASAGAC)?
Dogs have two anal sacs (often called “anal glands”) located just inside the anus at roughly the 4 and 8 o’clock positions. These sacs contain glands that produce secretions. ASAGAC is a malignant tumor that arises from those glandular cells. It often appears as a firm mass near the anus.
Even when the visible lump looks small, this tumor can be associated with enlargement of deep lymph nodes inside the pelvis. That is why careful staging—checking how far the disease has spread—is essential before deciding on the best treatment plan.
Common signs you may notice
- A lump next to the anus, swelling, bleeding, ulceration, or discharge
- Scooting, licking, discomfort, or pain around the rear end
- Thin stools, constipation, straining (especially if pelvic lymph nodes are enlarged and compress the rectum)
- Reduced appetite or energy (can be due to pain, infection, or systemic effects)
- Increased thirst/urination, nausea, weakness (may occur if blood calcium becomes elevated—“hypercalcemia”)
Why we don’t judge by appearance alone:Anal sac infections and inflammation can also cause swelling. We need an exam and appropriate testing to determine whether a mass is a tumor and whether there is spread to lymph nodes or other organs.
How do we diagnose it and stage the disease?
The goal is to answer three questions: “Is it cancer?”, “Has it spread?”, and “Is anesthesia and surgery safe for my dog?” A typical plan includes the following.
- Physical exam and rectal exam:We assess the mass, skin changes, pain, and the relationship to surrounding tissues. A rectal exam helps evaluate deep pelvic structures and whether the rectum is being compressed.
- Needle sampling (cytology) and/or biopsy:A fine needle sample may suggest a tumor, but a surgical specimen with pathology is often needed for definitive diagnosis and margin assessment.
- Bloodwork and urinalysis:We evaluate anemia/inflammation, liver and kidney function, electrolytes, and importantly blood calcium. Hypercalcemia affects both treatment planning and anesthesia safety.
- Imaging (chest X-rays, abdominal ultrasound, CT):We check for lung metastasis, evaluate pelvic lymph nodes (such as sublumbar/iliac nodes), and assess invasion into nearby tissues. CT is especially useful for deep pelvic lymph nodes and surgical planning.
- Cardiac assessment (as needed):For older dogs or dogs with heart disease, additional testing may reduce anesthesia risk.
Treatment options (the key is “local control + lymph node strategy”)
ASAGAC is treated by combining local control (removing or controlling the primary tumor) with a plan for potential lymph node involvement and recurrence risk. Your dog’s plan depends on staging results and overall health.
- Surgery to remove the anal sac tumor:When feasible, surgery is often the main treatment. The goal is complete excision with appropriate surgical margins.
- Pelvic lymph node management:If lymph nodes are enlarged, we may recommend sampling/removal, and/or additional therapies, depending on the case.
- Adjunct therapies:Chemotherapy, targeted therapy (for example, toceranib in selected cases), and/or radiation therapy may be discussed based on pathology and stage.
- Palliative/supportive care:If surgery is not appropriate, we focus on comfort, bowel function, and quality of life.
Important point:Treating only the visible mass may not be enough. Evaluating and addressing pelvic lymph nodes when indicated can be crucial for long-term control.
Anesthesia considerations
General anesthesia always carries some risk. We reduce that risk through pre-anesthetic testing, a tailored anesthesia plan, careful monitoring during the procedure, and structured post-operative care. With ASAGAC, we pay special attention to the dog’s overall condition (hydration, anemia/infection, kidney and liver function) and to hypercalcemia when present. High calcium levels can contribute to dehydration, nausea, kidney strain, and sometimes cardiac effects, so stabilization with fluids and supportive care may be recommended before surgery.
The anal region also has rich blood supply, and surgery can involve significant bleeding if not carefully managed. This is why precise hemostasis and continuous monitoring are essential.
What to expect after surgery (hospital stay, rechecks, home care)
After surgery, the top priorities are pain control, protecting the incision, and maintaining comfortable bowel movements. Mild swelling and discomfort are common for the first few days, and some dogs may strain or hesitate to defecate due to pain and tension in the area. In the hospital, we may use pain medication, antibiotics when appropriate, fluids, and bowel-supportive management such as stool softeners and diet adjustments.
At home, we typically use an e-collar to prevent licking, keep the area clean as directed, and monitor stool frequency and consistency, straining, bleeding, swelling, odor, and overall energy and appetite. Because this area is easily contaminated, gentle cleaning and close observation are important.
- Temporary constipation or straining can occur, but persistent or severe straining should be evaluated promptly.
- If bleeding increases, swelling worsens rapidly, pus appears, pain is severe, or appetite/energy drops, please contact your veterinarian as soon as possible.
- Suture removal timing depends on the incision and technique; we decide based on healing at recheck visits.
Possible complications
Complications cannot be reduced to zero, especially in the anal area. That is why careful technique, gentle tissue handling, reliable hemostasis, and attentive aftercare matter. Possible complications include infection, fluid accumulation (seroma), bleeding, wound dehiscence, painful defecation or constipation, and persistent discomfort around the anus. In some cases, depending on tumor location and extent, there can be risks involving the rectum and bowel function, which we evaluate and discuss in advance.
Signs that warrant prompt recheck:uncontrolled bleeding, rapidly increasing swelling, severe pain, repeated straining with little/no stool, fever-like lethargy, or a marked drop in appetite/energy.
Prognosis (what is the outlook?)
Prognosis depends on several factors: tumor size, pathology (including grade and surgical margins), whether lymph nodes are involved, how far the disease has spread, and which therapies are combined (tumor surgery plus lymph node management, with or without adjunct therapy). Because pelvic lymph node enlargement can be present even with a small external mass, imaging and staging before treatment play a major role in planning.
When treatment successfully controls the disease, many dogs experience improvement in bleeding, pain, and difficulty defecating, and quality of life can be very good. Because recurrence or metastasis can still occur, scheduled follow-ups are important. The interval depends on stage and treatment, but rechecks typically include a physical exam, bloodwork (including calcium when relevant), and imaging as needed to detect changes early.
Additional therapy (when recommended)
Based on pathology and staging, additional therapy may be recommended to reduce recurrence risk or control lymph node disease. Options can include chemotherapy, targeted therapy (such as toceranib in selected cases), and radiation therapy. The best choice depends on disease stage, other medical conditions, age, lifestyle, and what is realistic for ongoing care and rechecks.
If post-operative wound care is expected to be challenging or if infection risk is higher, certain surgical management strategies may be used, such as drain placement. If that may be needed, we discuss it before surgery so you know what to expect.
Frequently asked questions
- Can we just “watch it” if it’s a small lump?
Sometimes swelling is from infection or inflammation, but tumors cannot be ruled out by appearance. Early evaluation helps clarify the cause and can expand treatment options. - Will surgery make my dog unable to poop?
Temporary discomfort and straining can occur, but many dogs do well with pain control and stool management. Risk varies by tumor location and size, and surgical planning aims to protect bowel function. - We were told the pelvic lymph nodes are enlarged—what does that mean?
Pelvic lymph node enlargement is an important finding in ASAGAC. CT is often used to understand the anatomy, and we discuss whether sampling/removal and/or additional therapy is appropriate. - How often will we need rechecks after treatment?
Rechecks include incision monitoring, pathology review, discussion of any additional therapy, and ongoing follow-up exams and tests. The schedule depends on disease stage and treatment choices.
A simple place to add images later
You can add diagnostic images, surgical photos, or diagrams here later without breaking the flow of the article. If you add a short caption before each image, it becomes much easier for readers to follow.
If you want help deciding where each image best fits within the article, please share the order of images you plan to use and we can match them to the most relevant sections.
This section is intentionally kept simple so you can edit it freely.
Summary
- ASAGAC is a malignant tumor of the anal sac glands and may be associated with pelvic lymph node involvement.
- Treatment planning focuses on both the primary tumor and an appropriate strategy for lymph nodes.
- Anesthesia risk is reduced through testing, planning, and monitoring—hypercalcemia requires especially careful management.
- After surgery, incision care and monitoring bowel movements are key, and early contact for concerning signs supports safer recovery.
如果您发现狗狗肛门旁边出现“肿块”、肛门周围肿胀或出血——其中一种可能原因是来源于肛门囊的肿瘤。
本文可以帮助您了解
这是一篇面向饲主、尽量易懂但信息完整的说明,主题是肛门囊顶泌腺癌(ASAGAC):疾病概况、检查与分期的流程、治疗方法(手术、淋巴结处理、追加治疗)、麻醉风险、术后计划与居家护理、可能的并发症以及预后。即使不看原始文献,也能理解治疗思路与后续安排。
重要提示:肿块不一定“马上危及生命”,但也不能在没有检查的情况下就认为“可以先观察”。越早评估,往往越能保留更多治疗选择。
什么是肛门囊顶泌腺癌(ASAGAC)?
狗狗在肛门内侧左右各有一个肛门囊(常被称为肛门腺),大致位于“4 点钟与 8 点钟方向”。肛门囊内有分泌腺体,负责产生分泌物。肛门囊顶泌腺癌是一种来源于这些腺体细胞的恶性肿瘤,常表现为肛门旁边触到坚实的肿块。
即使外表看到的肿块并不大,也可能伴随骨盆深处的淋巴结肿大。因此,在决定治疗前,做“分期评估”(确认是否扩散、扩散到哪里)非常关键。
常见症状
- 肛门旁肿块、肿胀、出血、溃烂或分泌物
- 频繁舔咬、蹭地、坐姿异常、疼痛或不适
- 大便变细、便秘、用力排便(骨盆内淋巴结肿大压迫直肠时更常见)
- 精神食欲下降(可能与疼痛、感染或全身状态变化有关)
- 多饮多尿、恶心、无力(可能与“高钙血症”有关)
为什么不能只看外观判断?:肛门囊感染或炎症也会造成肿胀与疼痛。需要通过检查来确认是否为肿瘤,以及是否涉及深部淋巴结或其他部位。
需要做哪些检查?(诊断与分期)
检查的目标通常是回答三个问题:是不是肿瘤?有没有扩散?是否适合麻醉与手术?常见流程如下。
- 体检与直肠指检:评估肿块大小、皮肤情况、疼痛、与周围组织的关系。直肠检查可帮助判断骨盆深处是否有结构异常、直肠是否受压。
- 细针抽吸细胞学/活检:细胞学可提示肿瘤可能性,但很多情况下需要手术切除后的病理检查来最终确诊并评估切缘。
- 血液与尿液检查:评估贫血、炎症、肝肾功能、电解质,并特别关注血钙。若存在高钙血症,会影响治疗与麻醉计划。
- 影像学(胸片/腹部超声/CT):评估肺转移、骨盆深部淋巴结(如髂/腰下淋巴结等)是否肿大,以及是否侵犯周围组织。CT 对深部骨盆淋巴结评估与手术规划尤其有帮助。
- 心脏评估(按需):高龄或有心脏问题的狗狗,可能需要心电图或心脏超声,以降低麻醉风险。
治疗选择(关键是“局部控制 + 淋巴结策略”)
肛门囊顶泌腺癌的治疗通常需要把“原发灶控制”(肛门旁肿块)与“淋巴结/复发风险管理”结合起来。具体方案取决于分期结果与整体健康状况。
- 手术切除肛门囊肿瘤:在条件允许时,手术往往是主要治疗。目标是尽可能完整切除并获得合适的外科切缘。
- 骨盆内淋巴结处理:若淋巴结肿大,可能建议取样/切除,或结合其他治疗方式,视个案而定。
- 辅助/追加治疗:根据病理与分期,可讨论化疗、分子靶向药(例如在特定情况下使用托塞拉尼布等)及/或放射治疗。
- 姑息与支持治疗:若手术不适合,则以减轻疼痛、改善排便与生活质量为优先。
很重要的一点:只处理看得见的肿块可能不够。若分期提示骨盆内淋巴结受累,适当的淋巴结治疗往往对长期控制非常关键。
麻醉风险与注意点
全身麻醉一定存在风险,但我们可以通过术前检查、个体化麻醉方案、术中严密监测与术后管理,把风险尽量降到最低。对于肛门囊顶泌腺癌,尤其要关注整体状态(脱水、贫血/感染、肝肾功能)以及是否存在高钙血症。高钙血症可能导致食欲差、脱水、肾脏负担增加,甚至影响心脏,因此必要时会建议先进行补液与支持治疗,待状态更稳定后再手术。
另外,肛门周围血供丰富,手术过程中相对更容易出血,因此可靠止血与连续监测非常重要。
术后安排(住院、复诊与居家护理)
术后最重要的是控制疼痛、保护伤口,并让排便尽量顺畅。手术后几天内出现肿胀与不适是常见的,也可能因为疼痛与紧张而暂时排便困难。院内通常会进行止痛、必要时抗菌药、补液,以及帮助排便的管理(例如软便药与饮食调整)。
回家后建议佩戴伊丽莎白圈避免舔咬,并按医嘱保持清洁。请重点观察排便次数、软硬度、是否用力、出血或肿胀变化,以及精神食欲。由于该部位容易被污染,温和清洁与密切观察非常重要。
- 短期便秘或用力排便可能发生,但若持续用力、明显不适或排便困难加重,应尽快复诊。
- 若出血增加、肿胀迅速加重、出现脓液、疼痛明显,或精神食欲明显下降,请尽快联系医院。
- 拆线时间因伤口位置与缝合方式而异,会在复诊时根据愈合情况决定。
可能的并发症
肛门周围手术并发症无法做到“零”,因此术式选择、温柔的组织处理、可靠止血与术后护理都非常关键。可能出现的情况包括感染、积液(浆液肿)、出血、伤口裂开、排便疼痛或便秘、肛周持续不适等。根据肿瘤位置与范围,有时也可能涉及直肠与排便功能相关的风险,这些会在术前评估并说明。
需要尽快复诊的信号:出血止不住、肿胀迅速加重、疼痛明显、反复用力却几乎无便/不排便、精神萎靡像发热、食欲明显下降等。
预后(大概能恢复到什么程度?)
预后会因多个因素而不同:肿瘤大小、病理结果(恶性度与切缘)、是否有淋巴结转移、扩散范围,以及是否采用联合治疗(肿瘤切除 + 淋巴结处理,必要时再加上追加治疗)。由于外表肿块较小时也可能存在骨盆深部淋巴结肿大,因此治疗前的影像评估与分期对制定计划非常重要。
当治疗控制得当时,出血、疼痛与排便困难常会改善,生活质量可以明显提升。但该肿瘤仍可能复发或转移,所以治疗后需要定期复查。复查频率会根据分期与治疗内容调整,通常包括体检、血液检查(必要时含血钙)以及按需影像检查,以便尽早发现变化。
追加治疗(视情况而定)
根据病理与分期,有时会建议追加治疗来降低复发风险或控制淋巴结病灶,例如化疗、分子靶向药(在特定个案中可能考虑托塞拉尼布等)、放射治疗等。选择哪一种更合适,需要结合分期、共病、年龄、生活方式与复诊可行性一起讨论。
如果预计术后伤口护理难度较高或感染风险较大,手术管理上也可能采用一些策略,例如放置引流管等。如有这种可能性,会在术前一并说明,让您对术后安排有充分预期。
常见问题
- 肛门旁的小肿块可以先观察吗?
有时是感染或炎症,但仅凭外观无法排除肿瘤。尽早检查能更快明确原因,也更可能保留更多治疗选择。 - 手术会不会导致以后不能排便?
术后短期不适与用力排便可能发生,但很多狗狗在止痛与软便管理下能逐渐恢复。风险与肿瘤位置与范围有关,术前评估与术式规划会尽量保护排便功能。 - 医生说骨盆深处淋巴结肿大,这意味着什么?
骨盆内淋巴结肿大是本病的重要所见。CT 常用于了解解剖关系,并讨论是否需要取样/切除及是否需要配合其他治疗。 - 治疗后需要多久复查一次?
复查包含伤口评估、病理结果说明、必要时追加治疗讨论,以及后续长期随访。复查间隔会根据分期与治疗方案调整。
后续添加图片的位置
您可以在这里后续加入检查影像、手术照片或示意图,不容易破坏文章结构。建议在每张图前加入一两句简短说明,读者会更容易理解。
如果您希望把图片更精确地放到最匹配的段落附近,只要告诉我您准备使用图片的顺序,也可以帮您把内容与图片做更清晰的对应。
本段保持简洁,方便您自由修改。
总结
- 肛门囊顶泌腺癌属于恶性肿瘤,可能伴随骨盆深部淋巴结受累。
- 治疗计划需要同时考虑原发灶与淋巴结策略,必要时采用联合治疗。
- 麻醉风险可通过评估与监测降低;若有高钙血症,更需要细致的全身管理。
- 术后护理重点在伤口与排便观察,出现异常信号尽早联系医院,有助于更安全地恢复。