

診察時間
午前9:00-12:00
午後15:00-18:00
手術時間12:00-15:00
水曜・日曜午後休診

犬猫の膀胱結石と膀胱切開手術|麻酔リスクと術後ケアまでやさしく解説
わんちゃん・ねこちゃんの「膀胱切開手術」について、飼い主さん向けの説明と、後半に獣医療スタッフ向けの専門的なポイントをまとめました。
こんな症状はありませんか?
・血尿が出ている/おしっこがピンク色・赤色になっている
・何度もトイレに行くのに、少しずつしか出ない
・排尿時にキャンと鳴く、落ち着きがない
・まったく尿が出なくなり、ぐったりしている
これらは膀胱結石が原因で起きることが多く、放っておくと尿道閉塞や腎不全といった命に関わる状態につながることがあります。
膀胱切開手術ってどんな手術ですか?
膀胱切開手術は、膀胱の表面を小さく切開し、中にできた結石を直接取り出す手術です。
結石が膀胱の内側を傷つけることで起こる痛みや頻尿、血尿などのつらい症状を改善し、
尿の出口である尿道に石がつまってしまう「尿道閉塞」や、それに伴う腎不全を予防することが大きな目的です。
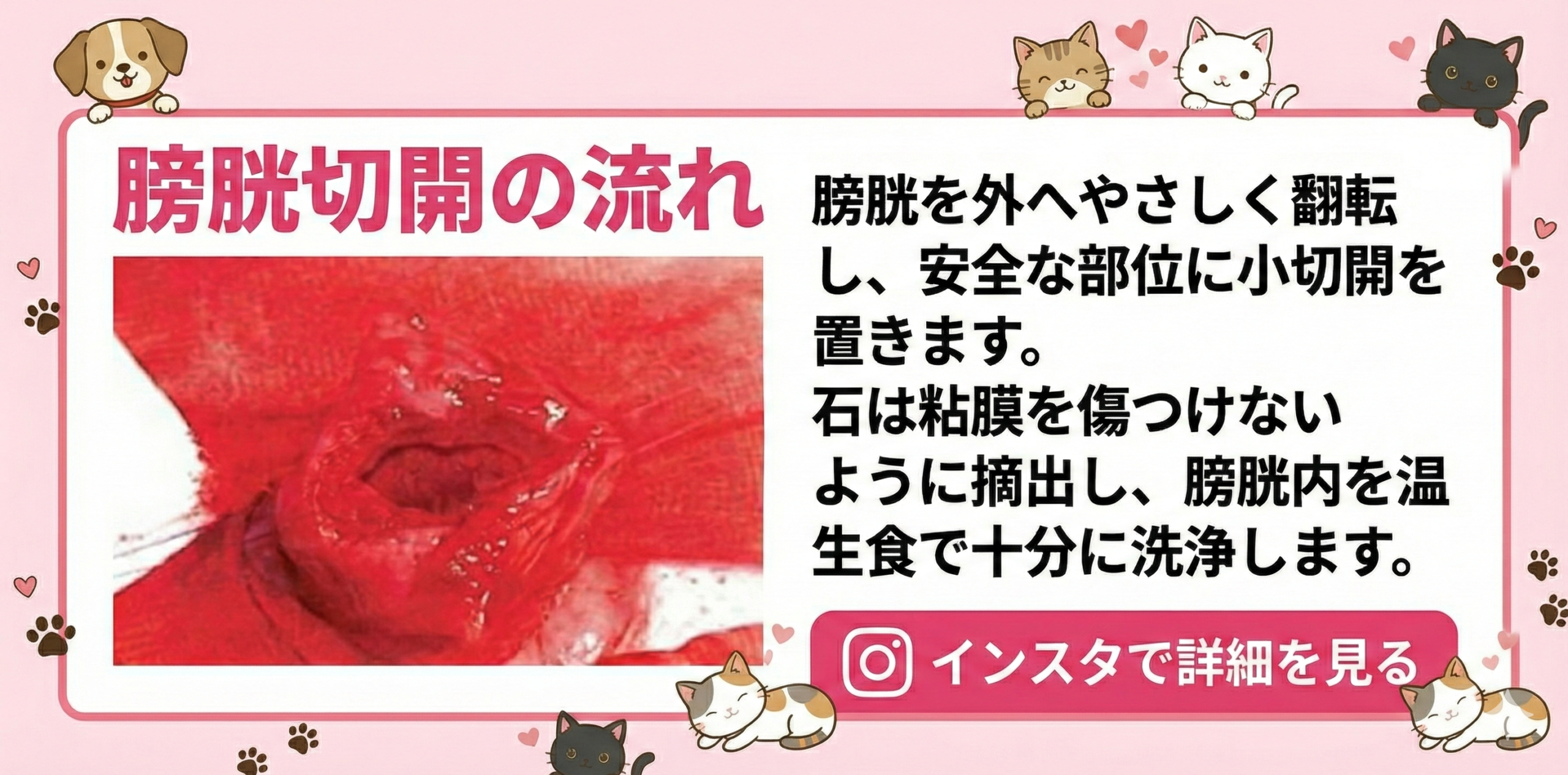
手術では、お腹を開けて膀胱をそっと体の外に持ち上げ、膀胱の血管や尿管を傷つけない位置に
小さな切開を入れて結石を取り出します。その後、膀胱を丁寧に縫い合わせて元の位置に戻します。
正しい位置に安全に切開を入れることと、しっかりと閉じて尿漏れを起こさないことが、膀胱切開手術で最も大切なポイントです。
どうして手術が必要になるのですか?
膀胱結石には、フードの変更だけで溶かせるタイプと、どうしても溶けないタイプがあります。
代表例として、ストルバイト結石は食事療法で改善することがありますが、
シュウ酸カルシウム結石はほとんど溶けず、基本的には物理的に取り除く必要があります。
結石が小さく数も少ない場合は、お薬や療法食で様子を見る選択肢もありますが、
大きくなった石や数が多い石は、将来尿道につまるリスクが高くなります。
レントゲン検査や超音波検査で、結石の大きさ・数・位置を確認し、
「内科管理で見ていけるか」「外科手術でしっかり取り除いた方が安全か」を判断していきます。
麻酔と手術のリスク、安全対策について
膀胱切開手術は全身麻酔が必要です。高齢であること、腎臓病や心臓病があること、
重度の感染や尿閉が続いていることなどは、麻酔リスクを高める要因になります。
そのため当院では、血液検査(腎臓・肝臓・電解質・炎症反応など)、
尿検査・尿培養検査、胸部レントゲンや心エコーなど、必要に応じた検査を事前に行い、
その子の状態に合わせて麻酔方法や点滴量、痛み止めの種類を細かく調整しています。
手術中は、心電図・血圧・体温・呼吸数・酸素濃度などをモニターで連続的に監視し、
変化があればすぐに対応できる体制を整えています。リスクがゼロになることはありませんが、
一つ一つのリスクをできるだけ小さくすることを心がけています。
手術当日の流れ
手術当日は、誤嚥防止のために前日の夜から絶食、当日朝からは絶水をお願いしています。
ご来院後に再度状態をチェックし、点滴用の静脈ルートを確保してから鎮静・麻酔導入を行います。
お腹の毛を刈り取って消毒し、正中切開でお腹を開けて膀胱を丁寧に取り出します。
周囲をガーゼで保護し、膀胱を温かい生理食塩水で湿らせながら、
血管や尿管から離れた安全な位置(膀胱の頂部・腹側)に小さな切開を入れて結石を取り出します。
結石の数や大きさにもよりますが、手術時間はおおよそ1〜2時間程度です。
結石をすべて取り除いたあと、膀胱内を十分に洗浄し、縫合部から尿が漏れないかどうかを確認します。
必要に応じて一時的な尿道カテーテルを留置し、お腹を閉じて手術は終了です。
術後の入院と、お家でのケア
手術直後は、点滴と痛み止め(注射や内服)を使用しながら、尿量・尿の色・体温・食欲などを細かく観察します。
尿道カテーテルを留置している場合は、閉鎖式のバッグにつなぎ、逆行性感染を防ぎながら膀胱内の血液や砂粒を洗い流します。
一般的には1〜3日ほどの入院で、状態が安定し、自力で問題なく排尿できることを確認してから退院となります。
お家に帰ってからしばらくは、激しい運動や階段の昇り降り、ジャンプは控えるようにしてください。
また、傷をなめたり引っかいたりしないよう、エリザベスカラーの着用をお願いすることが多いです。
おしっこの色が真っ赤になっていないか、排尿姿勢が長く続きすぎていないか、
痛そうに鳴いたり元気・食欲が落ちていないかをよく観察し、気になる変化があれば早めにご相談ください。
抜糸は、多くの場合術後10〜14日ごろに行います。
結石の検査と、再発を防ぐためにできること
取り出した結石は、可能な限り専門機関で成分分析を行います。
シュウ酸カルシウム結石、ストルバイト結石、尿酸塩結石、シスチン結石など、
成分によって再発予防の方法が大きく変わるためです。
例えばシュウ酸カルシウム結石では、食事療法で溶かすことはほぼできないため、
再発予防としては専用療法食による尿の性質の調整や、水分摂取量を増やすこと、
定期的な尿検査と腹部エコー検査による早期発見が重要になります。
ストルバイト結石では、適切な抗菌薬治療と感染コントロールに加え、pHを調整する療法食が役立ちます。
当院では、尿検査(比重・pH・潜血・細菌・結晶)や、画像検査を定期的に行いながら、
その子に合ったフードやサプリメント、生活スタイルをご提案し、
「手術して終わり」ではなく長期的なサポートを大切にしています。
よくあるご質問(Q&A)
- 手術は痛くないですか?
手術中は全身麻酔と鎮痛薬でしっかりと痛みをコントロールします。術後も注射や内服の痛み止めを併用し、なるべくストレスなく過ごせるように調整します。 - また結石ができてしまうことはありますか?
残念ながら、結石は一度取れば二度とできないというわけではありません。成分や体質によっては再発しやすい子もいますので、術後のフード管理と定期検査がとても大切です。 - シャンプーやお散歩はいつから再開できますか?
傷口がしっかりふさがるまではシャンプーは控えていただき、抜糸が終わってから再開するのが安心です。お散歩は、術後数日は短時間・平地中心から始め、徐々に元のペースに戻していきます。
ここからは、獣医療スタッフ向けの専門的なお話です
ここから先は、膀胱切開手術を担当する獣医師・愛玩動物看護師の方向けに、
解剖学的ランドマークと術式のポイント、術後管理と合併症対策を整理しています。
飼い主さまが読まれても問題ありませんが、やや専門的な内容を含みます。
雌:膀胱・尿管・子宮の位置と、安全な切開部位
雌犬・雌猫では、膀胱背側に子宮体〜子宮角が位置し、膀胱三角近傍に左右の尿管開口部が開口します。
膀胱切開は頂部腹側の無血管域で行うのが基本で、膀胱三角や尿道口付近の切開は、
出血・後の狭窄・膀胱尿管逆流のリスクが高くなるため避けます。
開腹時は、腹膜と膀胱漿膜との間を鈍的に剥離し、子宮動脈や膀胱動脈を一括して損傷しないよう層構造を意識します。
恥骨後縁近くからのアプローチでは、膀胱背側に走行する子宮動脈と膀胱背側血管網を誤って凝固・切断しないよう注意が必要です。
雄:膀胱・前立腺・尿道の解剖のポイント
雄では、膀胱は前立腺頭側に位置し、尿道は前立腺内を通過したのち骨盤腔尾側で腹側に急角度に屈曲して会陰部に至ります。
会陰部尿道カテーテルの挿入や逆行性尿道造影を行う際には、この屈曲をイメージしながら、適切なカテーテル径と角度で無理なく挿入することが重要です。
精管は膀胱頸部背側を横切り、射精管として前立腺内で尿道に合流します。
去勢済み個体でも遺残組織がみられることがあり、膀胱頸部付近での牽引や支持糸設置時に不要な損傷を避けるよう配慮します。
膀胱・前立腺・陰茎周囲の血管走行と注意点
- 膀胱動脈:内腸骨動脈から分岐する前・後膀胱動脈が膀胱頸部〜三角部を栄養します。頸部背側の結石や腫瘍へのアプローチ時には、この血管群の損傷による出血に注意します。
- 前立腺周囲静脈叢:豊富な静脈叢が存在し、浅・深陰部動脈や前立腺動脈の枝と交差します。膀胱頸部や前立腺背側での操作では、過度な牽引や鈍的剥離により大出血が生じる可能性があるため、圧迫止血と必要最小限の凝固を徹底します。
- 陰茎周囲血管:外陰部動脈および背側陰茎動脈が皮下を走行します。包皮切開やカテ固定のための縫合時には血流障害を起こさないよう、浅すぎず深すぎない針の深さと縫合間隔を心がけます。
膀胱切開の基本テクニック
開腹は通常、臍のやや尾側から恥骨前縁までの正中切開で行います。膀胱を腹腔外へ挙上し、
温生理食塩水で湿潤させたガーゼで周囲をパックして腹腔内汚染を予防します。
膀胱頂部腹側に頭尾側方向の支持糸を2〜4本掛け、操作野を安定させると同時に出血点の確認を容易にします。
切開は11番メスで小切開を入れ、メッツェンバウム剪刀で必要な長さまで延長します。
切開部位は膀胱三角および尿管開口部から十分距離をとり、背側血管網や頸部周囲静脈叢を避けます。
出血があればまず圧迫止血を行い、それでも止まりにくい場合は極小の凝固または結紮を追加します。
結石摘出と膀胱内洗浄のコツ
結石は鉗子で強くつまみ上げるのではなく、鋭匙やスプーン状の器具を用いてそっとすくい上げるように摘出します。
粗暴な把持は粘膜損傷や出血、結石破砕による取り残しの原因となるため避けます。
尿道内の砂粒は、膀胱からの逆行性洗浄で押し戻したのち再度膀胱内で回収します。
温生理食塩水で膀胱内を十分に洗浄し、指先と鋭匙で粘膜面をなぞりながら、砂粒や小結石の取り残しがないか確認します。
最後に膀胱内に生理食塩水を満たして軽く圧をかけ、縫合線からの漏れがないことを必ず確認します。
縫合法と縫合糸選択
縫合の目的は、尿漏れの防止・膀胱容量の保持・腔内異物量の最小化です。
多くの症例で、単層全層連続縫合または単層単純結節縫合で十分な強度が得られます。
感染尿症例では、膀胱腔内に露出する糸量を減らすために単層全層縫合を選択することが多いです。
縫合糸は、モノフィラメント吸収糸(例:PDS、Monocryl)が第一選択です。
感染やストルバイト結石症例で多芯糸を用いると、糸を核として新たな結石が形成されるリスクがあるため避けます。
糸のサイズは犬の体格や膀胱壁の厚さに応じて選択し、過度に太い糸は使用しません。
術後管理とモニタリング
- 尿路ドレナージ:尿道カテーテル留置を行う場合は閉鎖式システムとし、逆行性感染を防ぎながら膀胱内洗浄を行います。カテーテル抜去後の自力排尿を必ず確認します。
- 疼痛管理:オピオイド・NSAIDs・局所ブロックなどを組み合わせ、体格や腎機能に応じて投与量を調整します。
- 検査のフォロー:CRPや白血球数、BUN・クレアチニン、電解質を術前〜術後にかけてモニターし、腎前性要因や尿路感染の悪化がないか確認します。
想定される合併症と、その対策
- 術後尿漏れ・尿腹症:縫合線の破綻や縫合忘れ、過度な膀胱拡張が原因となります。術中の漏れテストを徹底し、術後は腹痛・元気消失・腹囲膨満などに注意します。疑わしい場合は腹水穿刺や造影検査で確認します。
- 術後尿路感染:留置カテーテル期間の長期化や不適切な閉鎖系管理がリスクです。必要最小限の留置期間とし、尿培養結果に基づいた抗菌薬選択を行います。
- 残石・再発:術中の洗浄不足や尿道内砂粒の取り残しにより早期再発が起こり得ます。十分な洗浄と、退院後の定期的な画像検査・成分分析に基づく食事管理が重要です。
まとめ:膀胱切開手術を安心して受けていただくために
膀胱切開手術は、適切な事前検査と麻酔管理、正しい解剖に基づいた切開部位の選択、丁寧な結石摘出と膀胱閉鎖、
そして術後のきめ細かなフォローがそろえば、わんちゃん・ねこちゃんの生活の質を大きく改善できる手術です。
飼い主さまには、不安な点やわからないことをそのままにせず、なんでもお話しいただきたいと思っています。
当院では、手術前から退院後の再発予防まで、ペットとご家族に寄り添いながら長くサポートしていきます。
This article explains bladder cystotomy for dogs and cats. The first part is for pet owners, and the latter part is for veterinary professionals.
Have you noticed any of these signs?
・Blood in the urine / urine that looks pink or red
・Frequent attempts to urinate but only small amounts come out each time
・Crying or acting restless when urinating
・No urine coming out at all and your pet seems weak or lethargic
These signs are often caused by bladder stones. If left untreated, they can lead to urinary blockage or kidney failure, which may become life-threatening.
What is bladder cystotomy?
Bladder cystotomy is a surgery in which a small incision is made in the wall of the bladder so that stones inside can be removed directly.
The main goals are to relieve painful symptoms such as blood in the urine and frequent urination, and to prevent stones from moving into the urethra,
where they can cause a complete blockage and secondary kidney failure.
During surgery, the abdomen is opened, the bladder is gently brought out of the abdominal cavity, and a small incision is made in a safe area that avoids blood vessels and the ureteral openings.
The stones are taken out, the bladder is sutured carefully, and then returned to its original position.
Choosing a safe incision site and closing the bladder securely to prevent urine leakage are the most important points in this procedure.
Why is surgery sometimes necessary?
Some types of bladder stones can be dissolved with special diets, while others cannot.
For example, struvite stones may respond to dietary management,
but calcium oxalate stones almost never dissolve and usually need to be removed physically.
If stones are small and few in number, it may be possible to monitor with diet and medication.
However, large or numerous stones carry a high risk of moving into the urethra and causing obstruction in the future.
X-rays and ultrasound are used to evaluate the size, number, and location of the stones and to decide
whether medical management is reasonable or surgical removal is safer.
Anesthesia risk and how we keep the procedure as safe as possible
Bladder cystotomy requires general anesthesia. Advanced age, kidney or heart disease, and severe infection or long-standing urinary obstruction
can all increase anesthetic risk. For this reason, we perform pre-operative tests such as
blood work (kidney and liver values, electrolytes, inflammatory markers),
urinalysis and urine culture, and chest X-rays or echocardiography when necessary.
Based on these results, we adjust the anesthesia protocol, fluid rate, and pain control for each individual patient.
During surgery, we continuously monitor ECG, blood pressure, body temperature, respiratory rate, and oxygen saturation.
If any changes occur, we can respond immediately. Risk can never be reduced to zero,
but our goal is to minimize each risk factor as much as possible.
What happens on the day of surgery?
To reduce the risk of vomiting and aspiration, we usually ask for fasting from the night before
and no water on the morning of surgery. After check-in, your pet is examined again,
an intravenous catheter is placed, and sedation and induction of anesthesia are performed.
The abdominal hair is clipped and the skin is disinfected. A midline incision is made to open the abdomen, and the bladder is gently exteriorized.
The bladder is kept moist with warm sterile saline and surrounded with gauze to protect the abdominal cavity.
A small incision is then made on the safe, avascular area on the ventral surface near the apex of the bladder,
away from the trigone and ureteral openings, and the stones are removed.
Depending on the size and number of stones, surgical time is usually around 1–2 hours.
After all visible stones have been removed, the bladder is flushed thoroughly and the suture line is checked for leakage.
If needed, a temporary urinary catheter is placed. Finally, the abdomen is closed and the surgery is completed.
Hospitalization and home care after surgery
Immediately after surgery, we provide intravenous fluids and pain relief (injections and/or oral medication)
while closely monitoring urine output, urine color, body temperature, appetite, and comfort.
When a urinary catheter is in place, it is connected to a closed collection system to reduce the risk of infection
and to wash out blood clots and small stone fragments from the bladder.
In many cases, hospitalization lasts about 1–3 days. Your pet is discharged once their condition is stable
and they are able to urinate comfortably on their own.
At home, please avoid rough play, running, stairs, and jumping for a while.
To prevent licking or scratching at the incision, we usually recommend using an Elizabethan collar.
Watch for any bright-red urine, prolonged straining in the litter box or during walks,
crying due to pain, decreased appetite, or lethargy. If you notice any of these signs, contact us promptly.
Sutures are typically removed around 10–14 days after surgery.
Stone analysis and how to prevent recurrence
Whenever possible, removed stones are submitted to a laboratory for quantitative analysis.
The type of stone—such as calcium oxalate, struvite, urate, or cystine—greatly influences how we prevent recurrence.
For example, calcium oxalate stones cannot be dissolved by diet alone,
so prevention relies on special prescription diets that modify urine chemistry,
increasing water intake, and performing regular urinalysis and ultrasound to detect recurrence early.
For struvite stones, control of urinary tract infection with appropriate antibiotics,
along with a diet that adjusts urine pH, is particularly important.
We use regular urinalysis (specific gravity, pH, blood, bacteria, and crystals) and
imaging studies to decide on the best food, supplements, and lifestyle for each patient.
Our goal is not just to “finish the surgery” but to provide long-term support after surgery as well.
Frequently asked questions (Q&A)
- Will my pet feel pain during surgery?
During surgery, we use general anesthesia together with pain relief so that your pet does not feel pain.
After surgery, injectable and oral pain medications are given as needed to keep your pet as comfortable and stress-free as possible. - Can stones form again after they are removed?
Unfortunately, once a pet has formed stones, there is always a chance they may recur.
Some patients are more prone to recurrence depending on stone type and body chemistry, so diet management and regular check-ups after surgery are very important. - When can we resume bathing and normal walks?
Bathing should be postponed until the incision is fully healed and sutures have been removed.
Short, gentle walks on flat ground can usually be started a few days after surgery and then gradually increased back to the usual level.
From here on: information for veterinary professionals
The following section is intended for veterinarians and veterinary nurses involved in bladder cystotomy.
It covers anatomical landmarks, key surgical techniques, postoperative management, and complication control.
Pet owners are welcome to read, but the content is more technical.
Female anatomy: bladder, ureters, uterus, and safe incision sites
In female dogs and cats, the uterine body and horns lie dorsally to the bladder, and the ureters open into the bladder at the trigone region.
Cystotomy should be performed on the avascular ventral aspect near the apex.
Incisions near the trigone or proximal urethra increase the risk of bleeding, postoperative stricture, and vesicoureteral reflux and should be avoided.
During laparotomy, blunt dissection is used to separate the peritoneum from the serosal surface of the bladder,
taking care not to injure the uterine and vesical arteries as a unit.
When approaching near the pubic brim, surgeons must pay attention not to coagulate or transect the uterine artery and dorsal bladder vascular plexus on the dorsal surface.
Male anatomy: key points of the bladder, prostate, and urethra
In males, the bladder is located cranial to the prostate, and the urethra traverses the prostate before bending ventrally within the pelvic canal and running caudally to the perineal region.
When placing perineal urethral catheters or performing retrograde urethrography, it is important to visualize this curvature and use
an appropriate catheter size and angle so the catheter can be advanced smoothly without trauma.
The ductus deferens crosses the dorsal neck of the bladder and joins the urethra within the prostate as the ejaculatory duct.
Even in neutered animals, remnants can remain. When placing traction sutures or support sutures near the bladder neck, avoid unnecessary damage to these structures.
Vascular anatomy around the bladder, prostate, and penis
- Vesical arteries: Cranial and caudal vesical branches from the internal iliac artery supply the bladder neck and trigone.
When approaching stones or tumors near the neck, care must be taken to avoid significant bleeding due to damage of these arteries. - Periprostatic venous plexus: A rich venous plexus surrounds the prostate, interlacing with branches of the internal pudendal and prostatic arteries.
Excessive traction or blunt dissection near the dorsal aspect of the bladder neck and prostate can cause major hemorrhage,
so gentle handling, precise ligation, and careful coagulation are essential. - Penile vasculature: The external pudendal and dorsal penile arteries travel subcutaneously along the penis.
During preputial incisions or catheter fixation sutures, take care with needle depth and spacing to avoid compromising blood flow.
Basic technique of bladder cystotomy
A standard approach is a ventral midline celiotomy from slightly caudal to the umbilicus to the cranial brim of the pubis.
The bladder is exteriorized, and the abdominal cavity is protected with warm saline-soaked laparotomy sponges.
Two to four traction sutures are placed on the ventral apex in a cranial-caudal direction,
which stabilizes the surgical field and facilitates identification of bleeding points.
A small stab incision is made with a #11 blade and then extended to the desired length using Metzenbaum scissors.
The incision should be located sufficiently distant from the trigone and ureteral openings and away from the dorsal vascular plexus and neck vessels.
Initial hemostasis is achieved with digital pressure; if persistent, minimal coagulation or ligation is added.
Tips for stone removal and bladder lavage
Stones should not be grasped aggressively with forceps. Instead, use a curette or spoon-shaped instrument to gently scoop them out.
Rough handling can damage the mucosa, cause bleeding, and crush stones into fragments that are easily left behind.
Sand and small calculi in the urethra are flushed retrograde back into the bladder and then removed.
The bladder is thoroughly lavaged with warm saline. The mucosal surface is palpated and visually inspected
to detect any residual sand or small stones. Finally, the bladder is filled with saline and mild pressure is applied
to confirm that there is no leakage from the suture line.
Suture pattern and suture material selection
The goals of closure are to prevent urine leakage, maintain bladder capacity, and minimize intraluminal foreign material.
In most cases, a single-layer appositional pattern—either simple continuous or simple interrupted—provides adequate strength.
In infected urine, a single-layer full-thickness pattern is often chosen to reduce the amount of exposed suture inside the lumen.
Monofilament absorbable sutures (e.g., PDS, Monocryl) are the first choice.
In cases with infection or struvite stones, braided sutures can act as a nidus for new stone formation and should be avoided.
Suture size is selected based on body size and bladder wall thickness; excessively large diameter should be avoided.
Postoperative management and monitoring
- Urinary drainage: When a urethral catheter is left in place, use a closed collection system and perform bladder lavage as needed while minimizing retrograde infection. Confirm spontaneous urination after catheter removal.
- Pain control: Combine opioids, NSAIDs, and local techniques as appropriate, adjusting doses according to body size and renal function.
- Laboratory follow-up: Monitor CRP or WBC count, BUN/creatinine, and electrolytes before and after surgery to detect prerenal factors and worsening urinary tract infection.
Expected complications and how to manage them
- Postoperative urine leakage / uroabdomen: This may result from failure of the suture line, missed suture holes, or excessive bladder distension.
Intraoperative leak testing is essential, and postoperatively clinicians should watch for abdominal pain, lethargy, and abdominal distension.
If suspected, perform abdominocentesis or contrast studies. - Postoperative urinary tract infection: Prolonged catheterization and inadequate closed-system management are major risk factors.
Keep the duration of catheterization as short as possible and choose antimicrobials based on urine culture and sensitivity. - Residual stones and early recurrence: Inadequate lavage or persistence of sand within the urethra can lead to early recurrence.
Thorough intraoperative flushing and, after discharge, regular imaging and diet adjustment based on stone analysis are crucial.
Summary: helping owners feel confident about bladder cystotomy
When supported by appropriate pre-operative assessment and anesthesia, correct anatomical understanding of incision sites,
gentle stone removal and secure bladder closure, and careful postoperative follow-up,
bladder cystotomy can greatly improve quality of life for dogs and cats.
We encourage owners to share any concerns or questions without hesitation.
Our hospital aims to support each pet and family not only through the surgery itself, but also in long-term management to prevent recurrence.
这篇文章介绍犬猫的膀胱切开手术。前半部分是给宠物主人看的说明,后半部分是提供给兽医及动物护理人员的专业内容。
您的爱宠有没有出现下面这些情况?
・尿液带血,或者颜色变成粉红色、红色
・频繁蹲厕所,但每次只能排出很少一点尿
・排尿时叫唤、烦躁不安
・完全排不出尿,整只动物精神沉郁、无力
这些症状常常与膀胱结石有关。如果放任不管,可能发展为尿道完全堵塞或肾功能衰竭,危及生命。
什么是膀胱切开手术?
膀胱切开手术是指在膀胱壁上做一个小切口,把里面形成的结石直接取出的手术。
主要目的,是缓解血尿、频尿等疼痛症状,并预防结石进入尿道造成“尿道梗阻”,以及由此引起的继发性肾功能衰竭。
手术时,首先打开腹腔,小心地把膀胱提到腹腔外,在避开血管和输尿管开口的安全区域做一个小切口。
取出结石后,再把膀胱仔细缝合,放回原位。
正确选择安全的切开位置,并牢固缝合膀胱以防止尿液渗漏,是这类手术最重要的要点。
为什么有时必须做手术?
有些膀胱结石可以通过特殊处方粮溶解,而有些则几乎无法溶解。
例如,鸟粪石(磷酸铵镁结石)有时可以靠饮食控制改善,
而草酸钙结石几乎不能通过饮食溶解,通常需要通过手术物理取出。
如果结石体积很小、数量不多,可以在药物和处方粮的配合下先观察。
但是,当结石体积较大或数量较多时,将来移行到尿道造成堵塞的风险就会明显升高。
因此,我们会通过X光与超声检查评估结石的大小、数量及位置,
再判断是内科治疗即可,还是外科手术取石更安全。
麻醉与手术的风险,以及安全对策
膀胱切开手术需要实施全身麻醉。高龄、肾脏病或心脏病的存在,以及严重感染或长时间尿闭,
都会增加麻醉风险。因此,我们会在手术前进行
血液检查(肾功能、肝功能、电解质、炎症指标等)、
尿检与尿培养,必要时还会做胸片或心脏超声,
根据结果为每一位患者调整麻醉方案、输液量及镇痛方式。
手术过程中,会持续监测心电图、血压、体温、呼吸频率以及血氧饱和度,
一旦出现变化可及时处理。虽然无法把风险降到零,但我们会尽量降低每一项风险因素。
手术当天的一般流程
为减少呕吐和误吸的风险,我们通常会要求前一晚开始禁食,
手术当日早晨停止饮水。到院后再次检查身体状况,
放置静脉输液针后进行镇静和麻醉诱导。
剃除腹部毛发并充分消毒皮肤后,在腹中线切开腹腔,将膀胱轻柔地牵出。
用温热的无菌生理盐水浸湿纱布包裹膀胱周围,以保护腹腔环境。
接着在膀胱腹侧靠近顶端的无血管区域做小切口,避开膀胱三角区和输尿管开口,然后取出结石。
根据结石大小和数量不同,手术时间大约在1~2小时左右。
取出所有肉眼可见的结石后,用温生理盐水充分冲洗膀胱腔,并检查缝合线是否有漏尿。
如有需要,还会暂时留置导尿管。最后关闭腹腔缝合完毕,手术结束。
术后住院与在家的护理要点
手术后,会通过静脉输液和止痛药(注射及口服)来维持循环和镇痛,
同时密切观察尿量、尿液颜色、体温、食欲以及精神状态。
若留置导尿管,则接闭合式尿袋,一方面监测尿量,
另一方面冲洗膀胱内血块和细小结石碎片,以减少堵塞风险。
一般情况下,住院时间约为1~3天,待病情稳定且能够舒适自主排尿后安排出院。
回家后的一段时间内,请尽量避免剧烈运动、奔跑、上下楼梯和跳跃。
为防止舔咬伤口,通常会建议佩戴伊丽莎白圈。
需要特别留意尿液是否再次鲜红、排尿姿势是否持续时间过长、
是否因疼痛而叫唤、食欲和精神是否下降等,一旦发现异常请尽早联系医院。
皮肤缝线通常在术后10~14天左右拆线。
结石成分分析与复发预防
取出的结石,如果条件允许,会送到专业机构做定量成分分析。
草酸钙、鸟粪石、尿酸盐、胱氨酸等不同类型的结石,其复发预防策略差异很大。
例如草酸钙结石几乎无法靠饮食溶解,
因此预防重点在于通过处方粮调整尿液性质、增加饮水量,
并定期做尿检和腹部超声,以便及早发现复发。
对于鸟粪石结石,除了需要使用合适的抗生素控制尿路感染外,
调整尿液pH值的处方粮也十分关键。
我们会根据定期的尿检(比重、pH、潜血、细菌及结晶)和
影像检查结果,为每一只动物制定合适的日粮、补充剂和生活方式建议。
目标不仅是“完成这台手术”,而是在术后长期陪伴,帮助降低复发风险。
常见问答(Q&A)
- 手术过程中会疼吗?
手术时会使用全身麻醉,并配合镇痛药,让动物在手术中不会感到疼痛。
术后也会根据情况使用注射或口服的止痛药,尽量让它舒适、减轻压力。 - 取出结石后,还会再长吗?
很遗憾,结石并不是取出一次就永远不会再长。
根据结石类型和体质不同,有些个体复发风险较高,
因此术后的饮食管理和定期复查非常重要。 - 什么时候可以恢复洗澡和正常散步?
在伤口完全愈合、拆线之前,应避免洗澡。
术后数日即可在平地上开始短时间轻松散步,随后可以逐渐恢复到原来的运动量。
从这里开始:给兽医及护理人员的专业内容
以下部分面向负责膀胱切开手术的兽医和爱宠护理人员,
总结了解剖学标志、手术要点、术后管理以及并发症处理。
宠物主人也可以阅读,但内容会更偏专业一些。
母犬母猫:膀胱、输尿管、子宫的位置与安全切开区域
在母犬母猫中,子宫体及子宫角位于膀胱背侧,输尿管在膀胱三角区开口进入膀胱。
膀胱切开应选择靠近膀胱顶端的腹侧无血管区。
膀胱三角或近端尿道附近的切口会增加出血、术后狭窄以及膀胱输尿管返流的风险,应尽量避免。
开腹时,可采用钝性分离,将腹膜与膀胱浆膜分开,
注意避免将子宫动脉和膀胱动脉整体损伤。
在接近耻骨前缘的操作中,要特别留意膀胱背侧的子宫动脉和膀胱背侧血管网,
避免误凝或切断。
公犬公猫:膀胱、前列腺及尿道的解剖要点
公犬公猫的膀胱位于前列腺头侧,尿道穿过前列腺后在骨盆腔内向腹侧急剧弯曲,再延伸到会阴部。
进行会阴尿道导尿或逆行尿道造影时,需要在脑中描绘这种弯曲形态,
选用合适的导尿管直径与插入角度,以便在不造成损伤的前提下顺利通过。
输精管在膀胱颈背侧横穿,并在前列腺内以射精管的形式汇入尿道。
即便已绝育,仍可能残留部分组织。
在膀胱颈部附近牵引或设置支持缝线时,应避免对这些结构造成不必要的损伤。
膀胱、前列腺及阴茎周围的血管走向与注意事项
- 膀胱动脉:来自内髂动脉的前、后膀胱动脉为膀胱颈及三角区供血。
在处理颈部附近结石或肿瘤时,应充分认识这些血管,避免粗暴操作导致严重出血。 - 前列腺周围静脉丛:前列腺周围存在丰富的静脉丛,并与阴部动脉和前列腺动脉分支交织。
在膀胱颈和前列腺背侧操作时,过度牵拉或钝性分离容易引起大出血,
因此需要轻柔操作、准确结扎,并将电凝控制在最小范围内。 - 阴茎周围血管:外阴部动脉及阴茎背动脉沿皮下行走。
进行包皮切开或固定导尿管缝合时,针迹深度和间距要适当,避免影响局部血供。
膀胱切开的基本技巧
通常采用正中腹切口,从略偏脐尾侧到耻骨前缘。
将膀胱提到腹腔外,用温生理盐水浸湿的腹巾包裹,以防污染腹腔。
在膀胱顶端腹侧沿头尾方向放置2~4根牵引缝线,既稳定视野,又便于观察出血点。
使用11号刀片做小切口,再用Metzenbaum剪刀延长至所需长度。
切口应与膀胱三角和输尿管开口保持足够距离,同时避开背侧血管网及颈部血管。
止血首先通过指压完成,如仍不能止住,再辅以少量电凝或结扎。
取石与膀胱冲洗的小技巧
取石时不宜用血管钳等用力夹持结石,而应使用匙状刮勺等器械轻轻托起取出。
粗暴夹持会损伤黏膜、造成出血,并可能把结石夹碎形成细小碎片,增加残留风险。
对于尿道内的砂粒,可先逆行冲洗回膀胱,再一并取出。
用温生理盐水充分冲洗膀胱腔,同时用手指和器械仔细触摸、检查黏膜表面,
确保没有残留砂粒或小结石。最后向膀胱内注满生理盐水,轻轻加压,确认缝合线没有漏尿。
缝合方式与缝合线选择
缝合的主要目的,是防止尿液渗漏、保持膀胱容量,并尽量减少腔内异物量。
大多数病例采用单层贴合缝合(连续或单个简单结节)即可获得足够强度。
在感染性尿液病例中,为减少腔内暴露的缝线量,常选择单层全层缝合。
首选单股可吸收缝线(如PDS、Monocryl等)。
在伴有感染或鸟粪石的病例中,多股线容易成为新结石的核心,应尽量避免使用。
缝线粗细应根据体型和膀胱壁厚度选择,避免使用过粗的线。
术后管理与监测要点
- 尿路引流:如需留置导尿管,应使用闭合式系统,在尽量降低逆行感染风险的前提下进行膀胱冲洗。拔管后务必确认动物能顺利自主排尿。
- 疼痛控制:根据体重和肾功能,合理联合使用阿片类、NSAIDs以及局部封闭等镇痛手段。
- 实验室随访:在术前及术后监测CRP或白细胞、BUN/肌酐、电解质等指标,观察是否存在肾前性因素或尿路感染的恶化。
可能出现的并发症及对应策略
- 术后尿液渗漏/尿腹症:多由缝合线裂开、漏针孔或膀胱过度扩张造成。
术中必须进行漏水试验,术后需关注腹痛、精神沉郁、腹围膨大等表现;
一旦怀疑,应通过腹腔穿刺或造影检查确认。 - 术后尿路感染:长期留置导尿管以及不规范的闭合式管理是主要危险因素。
应尽量缩短导尿时间,并根据尿培养和药敏试验选择合适的抗菌药物。 - 残石与早期复发:术中冲洗不充分或尿道砂粒残留,容易导致早期复发。
因此应在手术中彻底冲洗,术后通过定期影像学检查和基于石成分分析的日粮调整来降低复发风险。
小结:让主人安心选择膀胱切开手术
在充分的术前评估与麻醉管理、基于正确解剖学的切开位置选择、
温和的取石和可靠的膀胱缝合,以及细致的术后随访的前提下,
膀胱切开手术可以显著改善犬猫的生活质量。
希望各位主人在感到不安或有疑问时,随时与我们沟通。
本院不仅重视手术本身,更重视术后的长期管理,与您一起守护爱宠的健康,减少结石的再次发生。