

診察時間
午前9:00-12:00
午後15:00-18:00
手術時間12:00-15:00
水曜・日曜午後休診

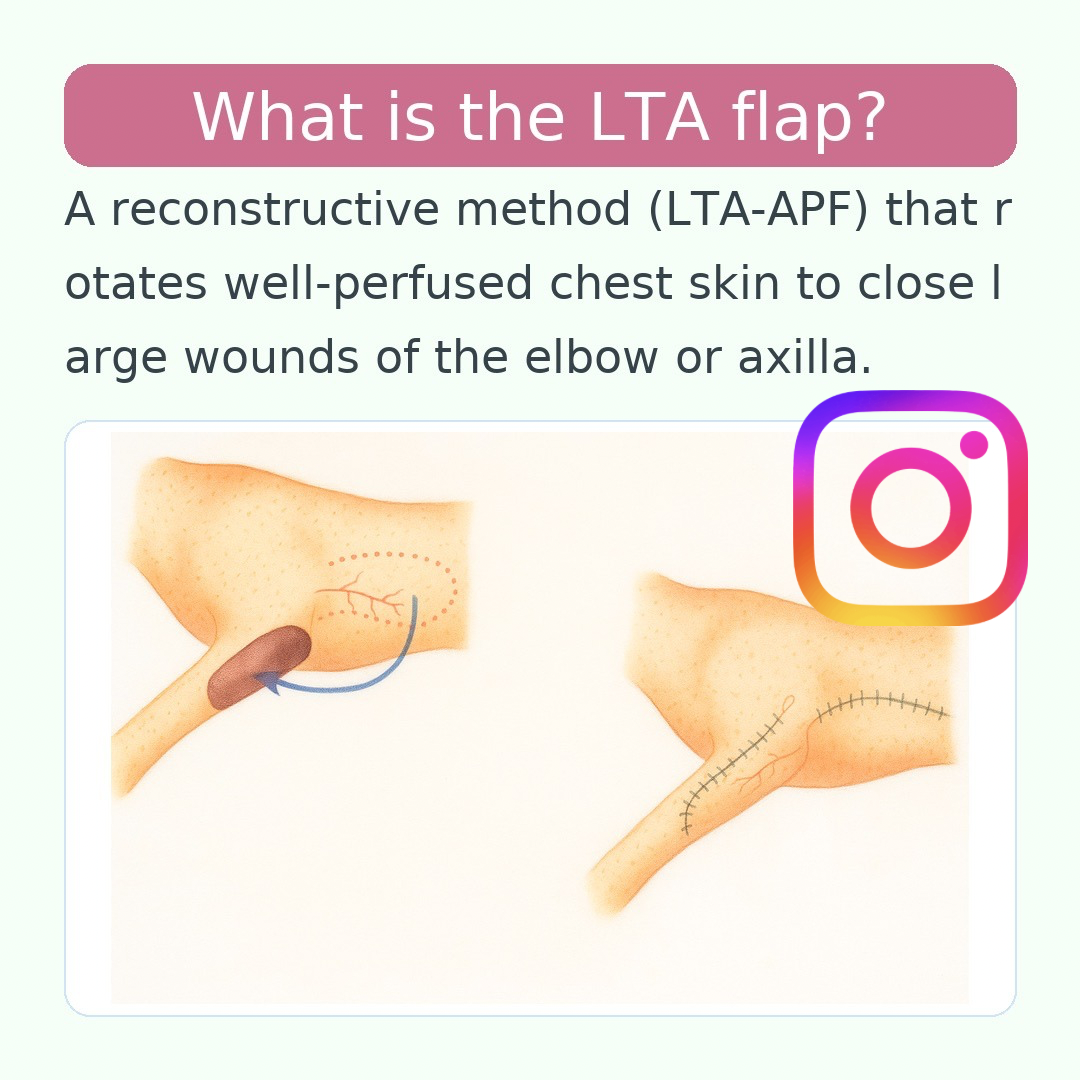
外側胸動脈軸上皮弁(Lateral Thoracic Artery Axial Pattern Flap; LTA-APF)前胸~上腕近位・肘周囲・前腕近位の皮膚欠損を閉鎖
外側胸動脈軸上皮弁(Lateral Thoracic Artery Axial Pattern Flap; LTA-APF)
を用いて、前胸~上腕近位・肘周囲・前腕近位の皮膚欠損を閉鎖するための手順を、解剖ランドマーク込みで「設計 → 採取 → 移動・縫合 → ドナー閉鎖 → 術後管理」の順に整理しました。
やさしい要点
・軸性皮弁なので安定した血流が得られ、大きめ欠損にも対応しやすい。
・上腕三頭筋後縁の直後に沿う血管軸(外側胸動脈)を中心に、背腹対称で設計すると安全。
・肘部再建では約90°回転で届くことが多い。
解剖とランドマーク
- 供血血管:外側胸動脈(伴行静脈あり)。腋窩動脈から分岐し、腋窩リンパ節深部を通過、深胸筋(大胸筋深部)の背側縁に沿って尾側へ走行し、上腕三頭筋後縁の直後で皮下浅層に出る。
- 皮弁中心線(軸):触診で同定できる上腕三頭筋後縁直後の線(=LTA走行)。この線を皮弁の“軸”として設計。
- 到達範囲の目安:犬は肋骨弓(第8肋骨付近)まで、猫は最尾側肋骨近くまで安定灌流域。
- 回転点(pivot):腋窩でLTAが浅層化する部。ここを中心に~約90°回転が可能。
① 術前計画・マーキング
- 体位:健側下の側臥位。患肢は軽度外転+前方牽引で腋窩を開く。
- Dopplerで軸確認:腋窩の尾側でLTA拍動を確認(上腕三頭筋後縁・深胸筋背側縁の交点付近)。
- 長さ設定:前縁=上腕三頭筋後縁/後縁=肋骨弓を基準に、欠損に対して1–2cmの余裕を取る。
- 幅設定:腹側縁を乳腺列外側~腹正中のやや外側に置き、LTA中心線から背腹対称になるよう背側縁を決める。
- 回転方法:pivotを中心に回転するか、腋窩~上腕内側にブリッジ切開を作ってねじれを回避するかを選択。
- サイズ参考:猫:平均およそ8.7 × 15.5 cmで全域灌流。犬:体格に応じて上記ランドマーク内で拡縮。
② 採取(ディセクション)
- 切開層:皮膚→皮下→体幹皮筋まで一気に。皮弁に体幹皮筋を必ず含める。
- 剥離層:体幹皮筋の深層面(筋膜下)で尾側→頭側へ鈍鋭併用。
- 基部の温存:腋窩近くでLTA+伴走静脈を視認し、2–3cm幅の脂肪・結合織ごと温存。結紮/焼灼は最小限。
- 穿通枝:1–2cm間隔で多数。遠位ほど細いので先端は厚めに保持。
- 保護:皮弁下面は湿ガーゼで乾燥防止。ドナー面は最小限止血。
③ 皮弁の移動と縫合
- A. 回転移動:pivotで~90°回転。屈曲・捻転ゼロを指で確認。張力が強い場合は受容床に緩解切開。
- B. ブリッジ切開:腋窩~上腕内側に皮膚橋を作り、皮弁を通してねじれ回避。
- C. 島状化:皮膚橋を切断し血管柄のみで移動範囲拡張(上級者向け)。
- 縫合:受容床を最終デブリ後に洗浄し、皮下(3-0~4-0吸収糸)→皮膚(3-0~4-0モノフィラ)で低張力・層々縫合。
- タッキング:必要部位は筋膜へ数点固定して剪断力を軽減。
- ドレーン:皮弁直下は縫い潰さず、ペンローズ or 吸引を24–72時間留置。
④ ドナー部の閉鎖
- 可能なら一次縫合。張力が強い場合は進展切開、または自由植皮(例:肩甲部)を追加。
⑤ 術後管理と合併症
- 固定:肘~前腕に及ぶ場合はスパイカ包帯で可動制限。過度な圧迫は避ける。
- 基本管理:保温・鎮痛・必要に応じ抗菌。創は清潔乾燥を維持。
- モニタリング:色調・温度・毛細血管再充満。暗赤色+冷感は静脈うっ血(包帯圧/屈曲/ねじれ)を疑い是正。
- 合併症:遠位壊死、漿腫、感染、縫合離開。軸性皮弁はランダム皮弁より生存率が高いが、過伸張・柄の屈曲でリスク増。
適応の目安
- 肘後部潰瘍・肘部変性創
- 上腕~前腕近位の外傷性欠損
- 腋窩周囲~前胸壁の欠損(~90°回転での到達が目安)
サイズの実感値(参考)
- 犬:頭尾方向は上腕三頭筋後縁~肋骨弓内で可及的に確保。幅はLTA軸の左右対称を基本に調整。
- 猫:平均約8.7 × 15.5 cm。90°回転で上腕~前腕近位へ到達可能。
手術のコツ(Pearls)
- 軸から等距離の背・腹縁で左右対称に設計 → 辺縁壊死を減らす。
- 基部の扱いは繊細に:腋窩近位は太い穿通枝が多い。圧挫・牽引を最小限に。
- 厚めに挙上+体幹皮筋を含めることでランダム化を防ぐ。
- 皮弁直下は縫い潰さずドレーンで漿腫対策。
- 到達が不足する時はまずブリッジ切開を検討(島状化は上級手技)。

Lateral Thoracic Artery Axial Pattern Flap (LTA-APF)
— step-by-step workflow to close defects around the cranial thorax, axilla, proximal brachium, elbow region, and proximal antebrachium:
Design → Harvest → Transfer & Closure → Donor Closure → Post-op Care.
At a glance
• As an axial flap, it provides reliable perfusion and tolerates larger defects than random flaps.
• Design the flap symmetrically around the vascular axis just caudal to the triceps long head.
• For elbow reconstruction, a ~90° rotation usually reaches the defect.
Anatomy & Landmarks
- Source vessels: Lateral thoracic artery with comitant vein, branching from the axillary artery, coursing caudally along the dorsal border of the deep pectoral, then becoming superficial just caudal to the triceps.
- Axis line: Palpable line immediately caudal to the triceps; use this as the flap’s center line.
- Reach (safe angiosome): In dogs, extends caudally to the costal arch (≈ 8th rib region). In cats, perfusion often reaches to the most caudal ribs.
- Pivot point: Where the LTA becomes superficial near the axilla—allows rotation of up to ~90°.
1) Pre-op Planning & Marking
- Positioning: Lateral recumbency, affected limb slightly abducted and protracted.
- Doppler mapping: Confirm LTA pulsation caudal to the triceps at the dorsal edge of the deep pectoral.
- Length: Cranial edge at the triceps caudal border; caudal edge up to the costal arch. Keep 1–2 cm design surplus.
- Width: Place the ventral edge along the lateral mammary line toward the paramedian abdomen; mirror this across the axis to obtain a bilaterally symmetric width.
- Transfer plan: Rotation about the pivot vs. bridge incision through the axilla/medial brachium to avoid pedicle twist.
- Typical sizes: Cats ~8.7 × 15.5 cm average; adjust for canine body size within the landmarks above.
2) Harvest (Dissection)
- Incision: Skin → subcutis → cutaneus trunci in one go; include the muscle with the flap.
- Plane: Dissect on the deep surface of the cutaneus trunci (subfascial), working from caudal to cranial.
- Pedicle preservation: Visualize the LTA and vein near the axilla and keep a 2–3 cm wide pedicle within surrounding fat.
- Perforators: Numerous at 1–2 cm intervals; keep the distal flap slightly thicker.
- Protection: Keep the deep surface moist; hemostasis on the donor bed is conservative.
3) Transfer & Skin Closure
- A. Rotation: Rotate up to ~90° at the pivot; confirm no kinking. Add relaxing incisions in the recipient bed if tension is high.
- B. Bridge incision: Create a skin tunnel to pass the flap while avoiding twist.
- C. Island flap: Divide the skin bridge and transfer on the pedicle alone (advanced option).
- Suturing: Layered low-tension closure — 3-0/4-0 absorbable in the subcutis, 3-0/4-0 monofilament in the skin.
- Tacking: Fix the flap to fascia at a few points to reduce shear.
- Drain: Do not obliterate the space; place a Pennrose or suction drain for 24–72 h.
4) Donor-site Closure
- Prefer primary closure when possible; otherwise use advancement incisions and/or STSG (e.g., from the scapular region).
5) Post-op Care & Complications
- Immobilization: If the flap crosses the elbow/antebrachium, use a spica bandage; avoid excessive compression.
- Routine care: Warmth, analgesia, and antimicrobials as indicated.
- Monitoring: Color, temperature, capillary refill; dark-red and cool suggests venous congestion → check bandage pressure, angulation, and twist.
- Complications: Distal necrosis, seroma, infection, dehiscence. Risk rises with over-stretching and pedicle kinking.
Indications
- Chronic pressure/degenerative wounds over the olecranon
- Traumatic defects of proximal brachium to proximal antebrachium
- Axillary & cranial thoracic wall defects (often reachable with ~90° rotation)
Practical Size (Reference)
- Dogs: Length from triceps caudal border to the costal arch; keep the design symmetric around the axis.
- Cats: About 8.7 × 15.5 cm on average; ~90° rotation usually reaches the elbow/proximal antebrachium.
Surgical Pearls
- Design equidistant dorsal & ventral borders from the axis to minimize marginal necrosis.
- Handle the pedicle gently—thick perforators arise proximally; avoid crush injury.
- Keep the flap thick with the cutaneus trunci to prevent “randomization”.
- Use a drain rather than closing the space under the flap.
- If reach is short, first consider a bridge incision; islanding is advanced.
外侧胸动脉轴型皮瓣(LTA-APF)
:用于修复前胸、腋窝、上臂近端、肘部及前臂近端皮肤缺损的标准流程:
设计 → 取皮瓣 → 转移缝合 → 供区关闭 → 术后护理。
要点速览
• 作为轴型皮瓣,灌注可靠,可覆盖较大的缺损。
• 以肱三头肌后缘正后方的血管轴为中心,背腹对称设计更安全。
• 肘部重建通常可通过约90°旋转到达。
解剖与标志
- 供血血管:外侧胸动脉及伴行静脉,自腋动脉分出,经深胸肌背侧缘向尾侧行走,于肱三头肌后缘正后方变为浅表。
- 轴线:可触及的肱三头肌后缘之后的线,作为皮瓣中心线。
- 覆盖范围:犬可达肋弓(约第8肋区域);猫通常可达最尾侧肋骨区域。
- 旋转枢纽:腋窝处外侧胸动脉变浅部位,允许约90°旋转。
① 术前计划与标记
- 体位:患侧朝上或下侧卧位,患肢轻度外展并前伸。
- Doppler定位:于肱三头肌后缘与深胸肌背缘的交界处探及外侧胸动脉搏动。
- 长度:前缘取肱三头肌后缘,后缘至肋弓;比缺损长度多预留1–2 cm。
- 宽度:腹侧缘沿乳腺外侧线/腹正中旁线,再以轴线为中心背腹对称确定背侧缘。
- 转移方式:以枢纽点旋转,或在腋窝~上臂内侧做桥式切开以避免血管柄扭转。
- 尺寸参考:猫平均约8.7 × 15.5 cm;犬按体型在上述标志范围内调整。
② 取皮瓣(离断)
- 切开层次:皮肤→皮下→皮肌一气呵成,并将皮肌包含于皮瓣内。
- 剥离平面:在皮肌深面(筋膜下)由尾向头钝锐结合分离。
- 血管柄保护:腋窝近端显露外侧胸动脉及伴行静脉,保留2–3 cm宽的脂肪组织带。
- 穿通支:约每1–2 cm一支;远端逐渐变细,故远端保留更厚。
- 保护措施:皮瓣深面湿纱布保湿;供区止血以最小化为宜。
③ 转移与缝合
- A. 旋转:围绕枢纽点约90°旋转,确认无折叠/扭曲;张力大时在受区做减张切开。
- B. 桥式切开:腋窝~上臂内侧建立皮肤桥,无扭转地牵引皮瓣通过。
- C. 岛状皮瓣:切断皮肤桥,仅依靠血管柄转移(高级操作)。
- 缝合:分层低张力缝合——皮下3-0/4-0可吸收线,皮肤3-0/4-0单丝。
- 固定:必要处将皮瓣缝至筋膜以减少剪切力。
- 引流:不缝闭皮瓣下死腔,放置橡皮引流/负压引流24–72小时。
④ 供区关闭
- 首选一期缝合;张力过大时可行进展切开或自由植皮(如肩胛部取皮)。
⑤ 术后护理与并发症
- 制动:跨越肘/前臂时应用肩托(Spica)包扎,避免过度加压。
- 常规护理:保温、镇痛、必要时抗菌。
- 观察:颜色、温度、毛细血管再充盈;若呈暗红且偏冷,考虑静脉淤血→检查包扎压力、角度与扭转。
- 并发症:远端坏死、浆液肿、感染、裂开;过度牵拉/血管柄折曲风险更高。
适应证
- 鹰嘴部慢性压力性/变性创面
- 上臂近端至前臂近端外伤性缺损
- 腋窝与前胸壁缺损(多可通过约90°旋转到达)
经验尺寸(参考)
- 犬:长度自肱三头肌后缘至肋弓;设计围绕轴线背腹等距对称。
- 猫:平均约8.7 × 15.5 cm;约90°旋转通常可达肘/前臂近端。
术中技巧(Pearls)
- 以轴线为中心背腹等距设计,减少边缘坏死。
- 近端穿通支较粗,操作轻柔避免压挫。
- 皮瓣厚取并包含皮肌,避免“随机化”。
- 皮瓣下方放置引流,不要缝闭死腔。
- 到达不足时先选桥式切开;岛状化属于高级策略。
