

診察時間
午前9:00-12:00
午後15:00-18:00
手術時間12:00-15:00
水曜・日曜午後休診

猫の巨大結腸症と結腸亜全摘|便秘が続く猫ちゃんの治療と手術のお話猫の巨大結腸症と結腸亜全摘|便秘が続く猫ちゃんの治療と手術のお話
猫の巨大結腸症(Megacolon)/結腸亜全摘のやさしいブログ解説
先にまとめ:長く続く便秘で結腸(太い腸)が伸びて拡がる病気です。まずは内科(便を柔らかく・腸を動かす・やさしい浣腸)から。改善しない/すぐ再発する場合は結腸亜全摘(結腸の大部分を切る手術)を検討します。
手術の成功率は90–95%。術後しばらくは軟便・回数増がみられますが、3〜6か月で落ち着くことが多く、生活の質が大きく改善します。
猫の巨大結腸症ってどんな病気?
- 腫瘍ではありません。長く続く便秘が原因で、結腸が拡がり、便を先へ送りにくくなる状態です。
- よくあるサイン:いきむ/少量しか出ない/食欲低下/嘔吐/元気がない など。
- レントゲンで診断:結腸の太さがL5(第5腰椎)長の約1.5倍以上だと重度と考え、治療方針を一緒に検討します。
まずは内科治療から(お家+病院)
- 便を柔らかく:ラクツロース/PEG3350(ポリエチレングリコール)で便に水分を含ませます。
- 腸の動きを助ける:シサプリド(個体差あり)。
- 病院でのやさしい浣腸:温かい生理食塩水+潤滑剤で便塊をふやかして排出を助けます。
- 注意:猫ではリン酸塩浣腸は危険(電解質異常)なので使用しません。
- 食事と水分:低残渣食で便の量を減らす/軽症では繊維食が合うことも。ウェットフードや給水器で水分をこまめに。

手術を考えるタイミングと術後のようす
- いつ検討?内科に抵抗/すぐ再発/重度拡張でQOLが落ちている場合に結腸亜全摘を選択肢に。
- 術後の一般的な経過:最初は軟便・排便回数増。多くは数週〜数か月(3〜6か月)で落ち着きます。
- すぐに連絡:ぐったり、発熱、強い腹痛、嘔吐が続く/食欲が戻らない、傷の腫れ・滲出が増える。
- 長期的には:再発便秘は少数で、食事・整腸剤・シサプリドで多くは管理可能。満足度の高い治療です。
お家でできるケアのポイント
- 水分アップ(ウェットフード、給水器、ぬるま湯のトッピング)。
- トイレ環境の見直し(数・清潔さ・段差を低くして行きやすく)。
- 2〜3日出ない、いきみが強い、ぐったり/食べない/吐く→早めに受診。
院内メモ(専門情報)|診断・適応基準
- 画像重度基準:最大結腸径 ≧ L5 椎体長の約1.5倍を実用閾値とする。
- 手術適応:内科(ラクツロース、シサプリド、温生食+潤滑浣腸、PEG3350、食事調整)に抵抗性/高頻度再発、著明な便塊貯留でQOL低下。
院内メモ|内科用量(代表)
- ラクツロース:0.5–1 mL/kg PO q8–12h(便性状で増減)。
- シサプリド(猫):0.1–0.5 mg/kg PO q8–12h(臨床では2.5 mg/頭 q8–12hを用いることが多い)。
- PEG3350:0.25–0.5 g/kg/day を分割投与(施設方針に従い少量から漸増)。
- 禁忌:リン酸塩浣腸。
- ※腎・肝、電解質、脱水の評価と合わせて安全域を確保。便性状・食欲・嘔吐の有無で用量微調整。
院内メモ|周術期管理(結腸亜全摘)
- 術前:脱水・電解質(特にK)補正、疼痛と悪心の制御、必要に応じ輸液・栄養サポート。
- 抗菌薬:清潔汚染手術として切皮30–60分前に投与、原則24h以内停止(例:cefazolin+metronidazole あるいは ampicillin-sulbactam、院内感受性に準拠)。
- 術後:早期鎮痛・早期経口(耐えれば低残渣→通常へ段階的に)、十分な水分。整腸剤/シサプリド併用可。
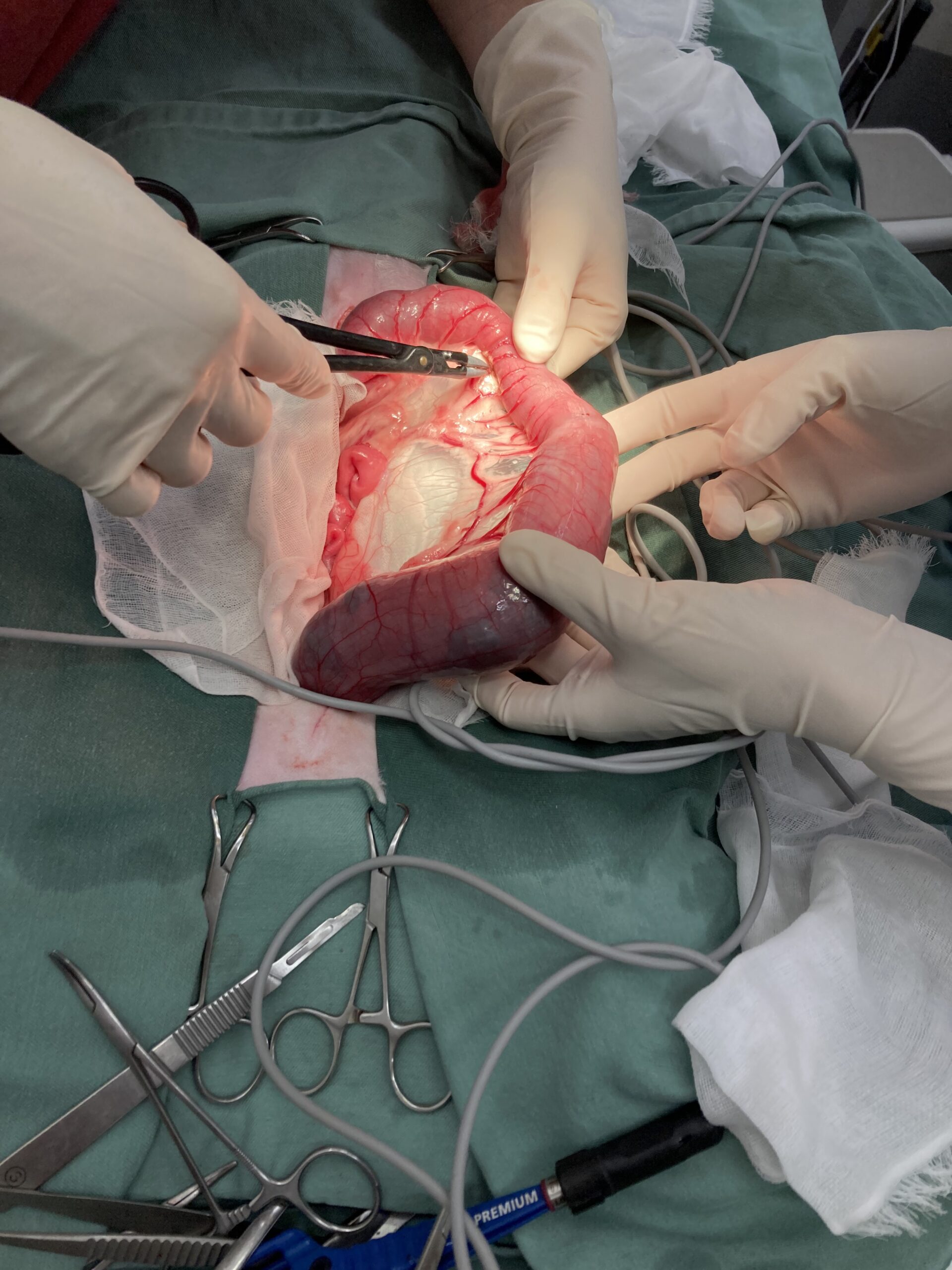
院内メモ|手術の実際(結腸亜全摘 90–95%切除目安)
- アプローチ:腹正中切開。結腸を温生食湿ガーゼで保護し外へ展開。
- 血管処理:前・中・後腸間膜動脈枝を結腸側で結紮し、回腸・盲腸の血行温存を意識。
- 回盲部温存:術後の液状便抑制・満足度に寄与する報告。
ただし病変・壊死・腫瘍が及ぶ場合は切除を優先。 - 吻合:端々吻合(単純結節 3-0 モノフィラメント)。
抗腸間膜側と腸間膜側に基準糸を置いてずれ防止、バイト3–4mm/間隔3mmを均等に。 - 径差調整:径差大→小径側をスパチュレーション。径差小→対腸間膜側に部分縦切開で口径調整。
- 補強:オメンタライゼーション/必要に応じ漿膜パッチ。
- チェック:リークテスト、血行(色調・拍動・蠕動)確認は必須。
院内メモ|合併症と対応・予後
- 縫合不全/漏出:術後3–5日がハイリスク。腹痛・発熱・腹水混濁で疑い→速やかに再評価(画像/腹腔穿刺)、必要に応じ再手術。
- 狭窄:細便・排便困難→造影・内視鏡で評価、バルーン拡張や再手術を検討。
- 便性状の変化:軟便・多便は数週〜数か月で順応が多い。食事・整腸剤・シサプリドで調整。
- 再発便秘:少数例。多くは食事・整腸・シサプリドで管理可能。
- 長期QOL:概ね良好。成功率90–95%、オーナー満足度は高い。
回盲部切除は液状便や満足度でやや不利とする報告あり(病変状況で選択)。
院外処方の目安(飼い主配布用ミニメモ)
- ラクツロース:0.5–1 mL/kg を 1日2–3回(便の柔らかさで微調整)。
- PEG3350:0.25–0.5 g/kg/日を分割(少量から開始)。
- シサプリド:0.1–0.5 mg/kg を 8–12時間毎(臨床では 2.5 mg/頭 q8–12h を用いることが多い)。
- リン酸塩浣腸は厳禁。
さいごに(ブログとしてのひとこと)
巨大結腸症は「がん」ではなく、丁寧な内科と必要に応じた手術で多くの猫が元気を取り戻せます。迷った時は一人で抱え込まず、ご家庭の生活スタイルや猫ちゃんの個性に合わせて、一緒に最適な方法を考えていきましょう。
当院では、内科・外科いずれの選択でも「痛みの少ない治療」「早期の食事再開」「ご家庭で続けやすいケア」を大切にしています。気になる症状があれば、早めにご相談ください。
(このページは飼い主さんが読みやすいように作成し、下段に専門情報を併記しています。診察時は最新の検査・状態に合わせて個別化します。)
よくある質問(Q&A)
- 手術しないとダメ? まずは内科を丁寧に行います。抵抗性/再発例で手術を検討します。
- 術後ずっと下痢? 初期は軟便〜多便でも、数週〜数か月で落ち着くことが多いです。
- 再発しない? 少数で便秘が戻ることがありますが、多くは食事・整腸剤・シサプリドで管理可能です。
- お薬はいつまで? 便性状と全身状態で調整。自己判断で中止せず、通院時に相談を。
Feline Megacolon / Subtotal Colectomy – Gentle Blog Guide for Cat Owners
Quick summary: Feline megacolon is a condition where long-standing constipation causes the large intestine (colon) to stretch and dilate. We start with medical management (softening the stool, helping motility, gentle enemas). If this does not improve things or relapses soon, we consider subtotal colectomy (removing most of the colon).
Surgical success rates are around 90–95%. After surgery, soft stool and increased stool frequency are common for a while, but most cats settle within 3–6 months, and their quality of life improves greatly.
What is feline megacolon?
- It is not a tumor. It is a condition where long-term constipation leads to progressive dilation of the colon so that it can no longer move stool forward properly.
- Common signs: straining in the litter box, only passing small amounts, decreased appetite, vomiting, lethargy.
- Diagnosis on X-rays: we measure the diameter of the colon. When the colon diameter is about 1.5 times or more the length of the 5th lumbar vertebra (L5), it is considered severely dilated, and we discuss treatment options together.
Step 1 – Medical management (at home & in the hospital)
- Softening the stool: lactulose and PEG3350 (polyethylene glycol) are used to draw water into the stool and make it easier to pass.
- Helping gut motility: cisapride (response varies between individuals).
- Gentle enemas at the clinic: warm saline + lubricant to soften and break up the stool mass.
- Important: in cats, phosphate enemas are dangerous (can cause life-threatening electrolyte changes), so we do not use them.
- Diet and water: low-residue diets can reduce stool volume; in mild cases some cats do well on fiber diets. We always work to increase water intake with wet food, water fountains, and warm water added to meals.
When do we consider surgery, and what is recovery like?
- When to think about surgery? When medical treatment is ineffective, relapses quickly, or the colon is severely dilated and your cat’s quality of life is clearly reduced, subtotal colectomy becomes an important option.
- Typical postoperative course: in the beginning, soft stool and increased frequency are expected. Most cats stabilize over several weeks to a few months (often by 3–6 months).
- Contact us immediately if you see: marked lethargy, fever, strong abdominal pain, persistent vomiting, poor appetite, or increased swelling/discharge from the incision.
- Long-term outlook: recurrent constipation can occur in a minority of cases, but in many cats it can be managed with diet, probiotics/“gut-friendly” supplements, and cisapride if needed. Overall owner satisfaction with surgery is high.
- Success rate: approximately 90–95%.
Home care tips
- Encourage water intake (wet food, water fountains, adding warm water to meals).
- Optimize the litter box environment (enough boxes, kept clean, easy access with low edges).
- If your cat has no bowel movement for 2–3 days, strains a lot, is lethargic, not eating, or vomiting – please contact us early.
Clinic note (for vets) – Diagnosis & indications
- Radiographic severity: maximum colon diameter ≥ about 1.5 × L5 length as a practical threshold for severe dilation.
- Surgical indication: refractory or frequently recurrent constipation despite medical management (lactulose, cisapride, PEG3350, warm saline + lubricant enemas, diet), or large fecalomas causing significant QOL impairment.
Clinic note – Representative medical doses
- Lactulose: 0.5–1 mL/kg PO q8–12h (titrate to stool consistency).
- Cisapride (cats): 0.1–0.5 mg/kg PO q8–12h (in practice, ~2.5 mg/cat q8–12h is commonly used).
- PEG3350: 0.25–0.5 g/kg/day divided (often starting at a low dose, then increasing as tolerated per clinic protocol).
- Contraindication: phosphate enemas.
- Always interpret doses in the context of renal/hepatic status, electrolytes, hydration, appetite, and vomiting. Adjust to the individual cat’s stool quality and clinical response.
Clinic note – Perioperative management (subtotal colectomy)
- Pre-op: correct dehydration and electrolytes (especially K), control pain and nausea, provide fluid therapy and nutritional support as indicated.
- Antibiotics: treat as a clean-contaminated procedure; give the first dose 30–60 minutes before skin incision, and in principle discontinue within 24 hours (e.g., cefazolin + metronidazole or ampicillin–sulbactam, chosen according to local antibiogram).
- Post-op: early, adequate analgesia; early enteral feeding as tolerated (starting with low-residue diets, then transitioning to normal diets); maintain good hydration. Probiotics and cisapride can be used as adjuncts if indicated.
Clinic note – Surgical technique (subtotal colectomy, ~90–95% resection)
- Approach: ventral midline celiotomy; protect and exteriorize the colon with warm saline–moistened laparotomy sponges.
- Vascular ligation: ligate the cranial, middle, and caudal colic branches on the colic side, preserving blood supply to the ileum and cecum.
- Ileocolic/cecal preservation: preserving the ileocecal junction can reduce liquid stool and is associated with better owner satisfaction, when feasible. If diseased, necrotic, or neoplastic, resect as needed.
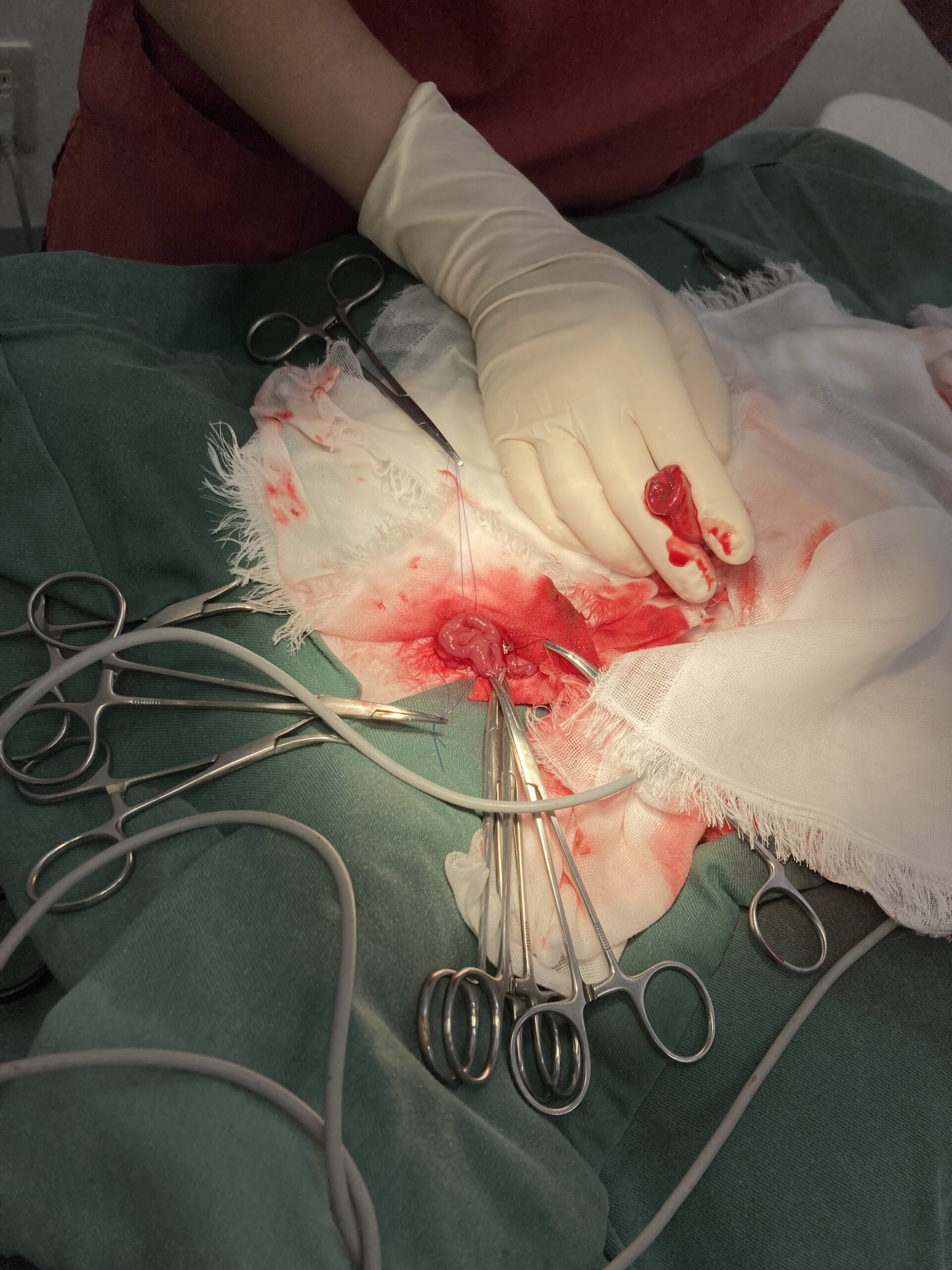
- Anastomosis: end-to-end anastomosis using simple interrupted sutures (3-0 monofilament). Place stay sutures on the anti-mesenteric and mesenteric borders to prevent rotation; maintain 3–4 mm bites, 3 mm spacing throughout.
- Diameter mismatch: for large discrepancies, perform spatulation of the smaller segment; for mild mismatch, a partial longitudinal incision on the anti-mesenteric border can help equalize luminal diameter.
- Reinforcement: omentalization and, if needed, a serosal patch.
- Final checks: leak testing of the anastomosis and careful assessment of perfusion (color, pulsation, peristalsis).
Clinic note – Complications, management, and prognosis
- Anastomotic dehiscence/leakage: highest risk around 3–5 days post-op. Suspect with abdominal pain, fever, and cloudy abdominal fluid; re-evaluate promptly (imaging/abdominocentesis) and consider revision surgery.
- Stricture: pencil-thin stool and renewed straining – evaluate with contrast studies/endoscopy; balloon dilation or revision surgery may be required.
- Changes in stool consistency: soft or more frequent stools are common for several weeks to months. Adjust diet, probiotics, and cisapride as needed.
- Recurrent constipation: occurs in a minority of cases; often manageable with diet and medical therapy.
- Long-term QOL: generally excellent, with 90–95% success rates and high owner satisfaction. Resection of the ileocecal junction has been associated with more liquid stool and slightly lower owner satisfaction in some reports, but final decisions depend on the extent of disease.
Take-home prescription guide (mini memo for owners)
- Lactulose: 0.5–1 mL/kg 2–3 times daily, adjusted to stool softness.
- PEG3350: 0.25–0.5 g/kg/day divided (start at a lower dose and increase gradually).
- Cisapride: 0.1–0.5 mg/kg every 8–12 hours (in many cats we start with about 2.5 mg/cat q8–12h and adjust).
- Phosphate enemas are strictly contraindicated in cats.
Closing thoughts
Feline megacolon is not a type of cancer. With careful medical treatment, and surgery when needed, many cats regain their comfort and energy. If you are unsure what to do, please don’t feel you have to decide alone. We will work with you to choose the best plan for your cat and your family’s lifestyle.
At our hospital, whether we choose medical or surgical treatment, we place great importance on gentle pain control, early return to eating, and home care that is practical for families. If you notice early signs of constipation or changes in your cat’s behavior, we encourage you to contact us sooner rather than later.
(This page is written in an owner-friendly style with technical notes added below. During consultations, we always individualize the plan based on the latest tests and your cat’s current condition.)
Frequently asked questions (FAQ)
- Is surgery always necessary? No. We always start with thorough medical management first. Surgery is considered for severe or refractory cases.
- Will my cat have diarrhea forever? No. It is common to have soft or frequent stools at first, but most cats improve over several weeks to months.
- Can constipation come back? It can recur in a minority of cases. Many of these can be managed with diet, probiotics, and cisapride.
- How long will my cat need medication? It depends on stool quality and overall health. Please do not stop medications on your own – we will adjust them together at follow-up visits.
猫的巨大结肠症 / 结肠次全切除手术|给铲屎官的温柔说明
先看重点:猫的巨大结肠症,是长期便秘导致结肠(大肠的一部分)被撑大、拉长的疾病。我们首先选择内科治疗(软化粪便、促进肠道蠕动、温和灌肠)。如果效果不好或很快复发,就会考虑结肠次全切除手术(切除大部分结肠)。
手术成功率大约在 90–95%。术后初期常见软便、排便次数增多,但多数猫在 3–6 个月内会逐渐稳定,生活质量明显提高。
什么是猫的巨大结肠症?
- 这不是肿瘤。是长期便秘导致结肠持续扩张,最后结肠无法有效推动粪便前行的一种状态。
- 常见症状:在猫砂盆里用力使劲但便便很少、排出的粪便量少或很硬、食欲下降、呕吐、精神沉郁等。
- X 光检查诊断:我们会测量结肠的直径。如果结肠直径约为第 5 腰椎(L5)长度的 1.5 倍及以上,通常认为是重度扩张,需要认真讨论下一步治疗方案。
第一步:内科治疗(在家 + 在医院)
- 软化粪便:乳果糖(Lactulose)以及 PEG3350(聚乙二醇)可以帮助粪便保留水分,变软、易排出。
- 促进肠道蠕动:西沙必利(Cisapride),不同个体的效果会有差异。
- 医院内温和灌肠:使用温热生理盐水 + 润滑剂,缓慢地将粪块软化、分解,帮助排出。
- 重要提醒:对猫来说,磷酸盐灌肠剂非常危险(会引起严重电解质紊乱),因此我们不会使用这类灌肠液。
- 饮食与水分:低残渣处方粮可以减少粪便量;轻度病例有时纤维粮也适合。但重度巨大结肠时,纤维过多反而可能让情况变糟。我们会尽量增加饮水量:湿粮、饮水机、在食物中加入温水等。
什么时候考虑手术?术后会怎样?
- 考虑手术的时机:如果内科治疗效果不佳、容易复发,或者结肠高度扩张、猫咪的生活质量明显下降,就会把结肠次全切除作为重要选项之一。
- 术后一般过程:早期常见软便、排便次数增加,这是预期之内的变化。多数猫会在几周到几个月(多在 3–6 个月内)逐渐稳定。
- 需要立刻联系医院的情况:明显精神沉郁、发热、严重腹痛、持续呕吐、食欲一直不恢复、切口肿胀或渗出增多等。
- 长远来看:少数猫会出现便秘复发,但很多情况下可以通过饮食调整、肠道益生类产品以及西沙必利等药物来控制。整体上,主人对手术的满意度较高。
- 成功率:约 90–95%。
在家可以做的小护理
- 想办法让猫多喝水(湿粮、饮水机、在食物里加入温水等)。
- 检查猫砂盆环境(数量够不够、是否干净、边缘高度是否方便进出等)。
- 如果 2–3 天没有排便、在猫砂盆里用力很明显、精神不好、不吃东西或呕吐,请尽早联系医院。
院内备注(专业)|诊断与手术指征
- X 光重度标准:最大结肠直径 ≥ 约1.5 × L5 长度,作为重度扩张的实用阈值。
- 手术指征:经过内科治疗(乳果糖、西沙必利、PEG3350、温生理盐水 + 润滑灌肠、饮食管理)仍然顽固或多次复发;或存在巨大的粪块导致明显生活质量下降。
院内备注|内科用药剂量(代表值)
- 乳果糖(Lactulose):0.5–1 mL/kg 口服,每 8–12 小时一次(根据粪便性状调整剂量)。
- 西沙必利(Cisapride,猫):0.1–0.5 mg/kg 口服,每 8–12 小时一次(临床上常以约 2.5 mg/只,每 8–12 小时为起始剂量,再根据情况调整)。
- PEG3350:0.25–0.5 g/kg/天,分次给药(通常从较低剂量开始,根据耐受情况逐渐增加,遵循各医院内部方案)。
- 禁忌:磷酸盐灌肠剂。
- 给药时需结合肾功能、肝功能、电解质、脱水情况以及食欲、呕吐等综合评估,并根据每只猫的粪便情况和反应来微调剂量。
院内备注|围手术期管理(结肠次全切除)
- 术前:纠正脱水和电解质紊乱(尤其是钾离子),控制疼痛和恶心,根据情况进行输液和营养支持。
- 抗生素:按“清洁污染手术”处理,在切皮前 30–60 分钟给首剂,原则上术后 24 小时内停药(例如头孢唑啉 + 甲硝唑,或氨苄西林/舒巴坦等,具体按院内药敏和指南选择)。
- 术后:尽早、足量镇痛;在耐受的前提下尽早恢复经口进食(先从低残渣饮食开始,再逐步过渡到普通饮食);保持良好的水化状态。必要时可加用益生菌类产品、西沙必利等。
院内备注|手术要点(结肠次全切除,切除约 90–95%)
- 手术入路:腹正中切开,使用温热生理盐水湿润纱布保护并牵出结肠。
- 血管处理:在结肠侧结扎前、中、后结肠动脉分支,同时注意保留回肠和盲肠的血供。
- 回盲部(回盲瓣)保留:如条件允许,保留回盲部有助于减少术后液体样粪便,并提高主人满意度;如果存在病变、坏死或肿瘤则以切除病变为先。
- 吻合方式:端端吻合,采用单纯间断缝合(3-0 单丝可吸收或不可吸收线)。在肠系膜侧及对侧各放置定位缝线防止扭转,整体保持进针间距约 3–4 mm,缝线间距约 3 mm。
- 管径不匹配的处理:当管径差异较大时,可对较细的一端做斜形切开(spatulation);当差异较小,可在对肠系膜侧做部分纵行切开以扩大腔径。
- 加固:大网膜覆盖(网膜包裹),必要时加做浆膜补片。
- 术毕检查:进行吻合口漏气/漏液测试,并仔细确认吻合段血供(颜色、搏动、蠕动)。
院内备注|并发症、处理及预后
- 吻合口裂开/漏出:术后3–5 天风险最高。若出现腹痛、发热、腹腔积液混浊等,要高度怀疑,需尽快影像学检查和腹腔穿刺评估,必要时二次手术修补。
- 吻合口狭窄:大便变细如铅笔样、排便困难时要怀疑,可通过造影或内镜评估,视情况行球囊扩张或再次手术。
- 粪便性状改变:软便、排便次数增多在数周至数月内比较常见,可通过调整饮食、益生菌、西沙必利等进行管理。
- 便秘复发:只见于少数病例,多数可通过饮食与内科治疗控制。
- 长期生活质量:整体预后良好,成功率约 90–95%,主人满意度高。有研究显示,切除回盲部的病例液体样粪便较多、满意度略低,但最终决定仍需结合病变范围。
给主人的用药小抄(院外处方小贴士)
- 乳果糖:0.5–1 mL/kg,每天 2–3 次,根据粪便软硬程度微调。
- PEG3350:0.25–0.5 g/kg/天,分次给药(通常从小剂量开始,逐渐加量)。
- 西沙必利:0.1–0.5 mg/kg,每 8–12 小时一次(临床上往往以约 2.5 mg/只、每 8–12 小时为起点,根据反应调整)。
- 绝对禁用:磷酸盐灌肠剂。
最后想对您说的话
巨大结肠症并不是癌症。通过细致的内科治疗,在需要时配合外科手术,很多猫都能重新恢复舒适、愿意吃饭、愿意活动的状态。如果您对“要不要手术”“这样治对不对”感到犹豫,请不要一个人扛着,我们会和您一起,根据猫咪和家庭的情况,找出最合适的方案。
在本院,无论是内科还是外科,我们都特别重视减少疼痛、尽早恢复进食,以及在家容易坚持的护理方式。如果您发现猫咪有早期便秘的迹象或行为变化,欢迎尽早与我们联系。
(本页面以便于铲屎官阅读为主,下方附带了一些专业备注。实际诊疗时,我们会结合最新检查结果和当下状态,为每一只猫制定个体化方案。)
常见问答(FAQ)
- 一定要做手术吗? 并不是。我们会先充分尝试内科治疗,只在重度或顽固病例中把手术作为重要选择。
- 术后会一直拉稀吗? 一开始软便、次数多是常见现象,但多数猫会在几周到几个月内逐渐稳定。
- 便秘还会不会再来? 少数猫可能再次出现便秘,但很多时候可以通过饮食、肠道保健品和西沙必利等药物来管理。
- 药要吃多久? 需要根据粪便状态和整体健康状况来调整。请不要自行停药,我们会在复诊时和您一起慢慢调整。